 RSS Feed
RSS Feed















 January 2nd, 2022
January 2nd, 2022  Awake Goy
Awake Goy By Luke Perry / 27 December 2021

We’re publishing a guest post by our in-house doctor today looking at the latest ICNARC data. This is the weekly audit of NHS ICUs. It only covers the period up to November 14th, but suggests that unvaccinated Covid patients in ICU are not placing an unmanageable strain on the NHS, as some health professionals have claimed. On the contrary, as of November 15th, there were only 400 unvaccinated Covid patients in ICUs across the whole of NHS England and they were outnumbered by vaccinated patients.
Today the Prime Minister will be making a decision on further measures to limit social interactions by British citizens. Information leaked from SAGE appear to indicate the ‘scientific advisers’ to the Government are pushing him to reinstitute more aggressive social controls in an effort to control the virus.
As Monday and Tuesday (the 27th and the 28th) are bank holidays, there will be no release of Covid related data on the NHS website. Therefore, the public will be able to see even less information than usual about the quantifiable evidence on which their liberty is being curtailed.
On Christmas Eve, the Intensive Care National Audit and Research Centre (ICNARC) released an updated weekly report containing useful new information. Readers may recall that until recently, ICNARC had not produced an audit of vaccination status in ICUs. We now have data up to November 15th and this week a more granular analysis has been published. The link to the report is here and the relevant pages are 44-48.
I urge readers to examine this report for themselves in tandem with my analysis as a guide to interpretation. There has been so much misinformation around vaccines and severe Covid on both sides of the argument that a high-quality ICNARC audit is invaluable in assessing quantifiable known facts about the situation.
Readers should note that all patients included in this audit were suffering from the Delta variant. The time period ends on November 15th, well before Omicron became established in the U.K. Therefore, the debate around whether Omicron is more or less severe than Delta is irrelevant for the purposes of this commentary.
Figure 27 on page 46 shows the changing proportions of vaccinated people in ICU units between May and November compared to vaccination status in the general U.K. population. Over this period vaccination uptake increased in the community from around 60% partially or double vaccinated in May to over 80% double vaccinated in November.

In May, 35% of the population were unvaccinated but 75% of ICU patients came from this cohort. By November about 15% of the population were unvaccinated but they accounted for 48% of the ICU population. The inference is that the risk of contracting severe Covid is substantially higher in the unvaccinated population than the vaccinated. Note there is no more recent data than November 15th, so we don’t have any evidence that the percentage of unvaccinated Covid patients in ICUs has increased since the Omicron variant hit.
Figure 28 on page 47 is interesting. It shows that London is significantly different to the rest of the U.K. in respect of unvaccinated admissions to ICU. In summary, London has a consistently higher percentage of unvaccinated patients in ICU compared to the rest of the U.K. – in November about 60% of London ICU Covid patients were unvaccinated compared to a range in the rest of the U.K. of between 40 and 50%. This probably reflects a lower vaccine uptake in the capital compared to the rest of the U.K. I will return to this point later.
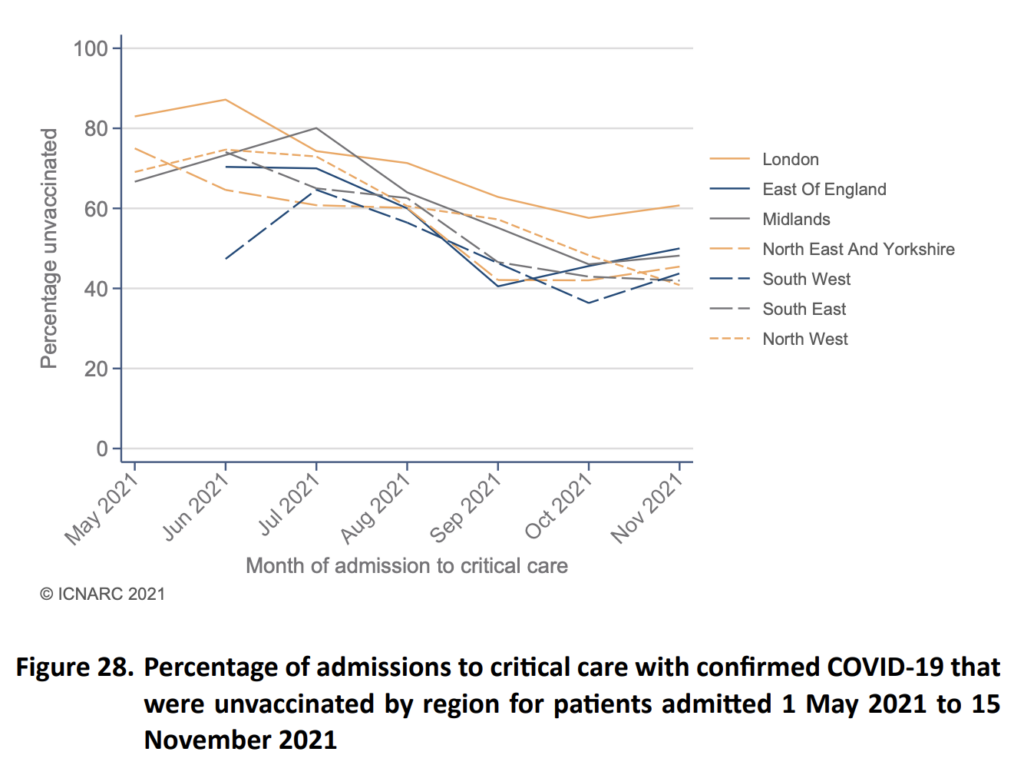
Table 16 on page 48 of the report is the most revealing new information. It provides a detailed analysis of vaccination status mapped to important demographic and clinical data around disease severity. I will take some time to unpick it for benefit of slightly nerdy ‘statos’ like myself!

The first observation is that unvaccinated patients on ICU tend to be younger than the double vaccinated (a mean age of 49 versus 65). There was a wider interquartile range in the unvaccinated than the vaccinated groups – this means that almost all of the patients in ICU under 40 were unvaccinated. There tended to be more females in the unvaccinated group (42% vs 33%).
Blacks, Asians and other ethnic minorities made up 33% of the unvaccinated cohort, but only 14% of the vaccinated group. This probably reflects lower vaccination uptake in these communities compared to the ethnically white British segment of the U.K. population.
Turning to socio-economic status (SES), there was a gradient observed in the two groups, with 64% of the unvaccinated group deriving from SES classes four and five compared to 48.4% in the vaccinated group. Again, this may reflect lower vaccine uptake in lower SES groups in the community.
The differences in physiological status are the most interesting data. In aggregate, vaccinated ICU patients were more likely to have serious comorbidities or vulnerabilities than unvaccinated patients. About 50% of the vaccinated patient group had serious pre-existing health conditions compared to 12.3% in the unvaccinated group.
Interestingly, the body mass indices were much the same in both groups. (I had expected the unvaccinated group to be fatter than the vaccinated, but this was not the case.) It was also interesting to see the physiological severity as measured by the requirement for early ventilation and the gas exchange ratios were the same across all groups. Finally, there was a significant group of pregnant or recently pregnant women in the unvaccinated cohort, not seen in the vaccinated group – this may reflect the age differences between the two groups.
So, in summary, my assessment of this information is as follows:
- Unvaccinated patients represented about half of patients in ICU compared to about 15% of the general population. Therefore, the risk of ICU admission in the unvaccinated is higher than the vaccinated population.
- Unvaccinated patients in ICU tend to be younger and healthier (before admission) than their vaccinated counterparts, half of whom were significantly unwell before contracting Covid.
- Unfortunately, ICNARC have not yet provided information around mortality rates between vaccinated and unvaccinated patients. I think it is probably reasonable to assume that unvaccinated patients, being generally younger and fitter than the vaccinated groups, are more likely to survive ICU.
- In quantitative terms, there were about 820 Covid patients in English ICUs in mid-November. By Christmas Eve this had fallen to 747. If 48% of patients are unvaccinated this represents about 400 unvaccinated ICU patients in England in November.
- London has a higher percentage of unvaccinated patients in ICU (60%) than the rest of the country. This may reflect skews to a younger demographic and a higher proportion of ethnic minorities, hence lower vaccine uptake in the capital.
- Reports in the media claiming that 90% of the ICU patients in London are unvaccinated are not supported by this audit – unless something has radically changed between November 15th and the end of December. My anecdotal information reports that there are some ICUs in London where the percentage of unvaccinated patients in ICU does approach 90%. These are hospitals in the East End and South East areas. My suspicion is that these higher rates are being extrapolated in the press as representative of the whole of the U.K. Actually, they are not even representative of the whole of London.
My final point goes to how this valuable information has been portrayed in the press. The ICNARC data provide good evidence of the protective effects of vaccination against Covid and the higher risk of being severely ill with Covid if one has not been vaccinated. Otherwise healthy patients who are unvaccinated are at higher risk of contracting severe Covid than their vaccinated peer group. However, the effect has been exaggerated by commentators in the mainstream media and the overall numbers are quite low (400 unvaccinated ICU patients in the whole of the U.K.).




_______________________________
If you are looking for solutions (lawyer, form, gathering, action, antidote, maybe this could help you:
HERE
If you want to fight back better:
https://childrenshealthdefense.org/child-health-topics/health-freedom/defender-days-sticker-gallery/
If you like our work please consider to donate :



Spike Protein Protocol
Glutathione (most important for body detoxification) or better
NAC = N-Acetyl-Cysteine 600-750mg (causes the body to produce glutathione itself)
Zinc
Astaxantin 5mg (also improves vision)
Quercetin
vitamin D3
Milk thistle (also liver and stomach protection)
Melatonin 1mg to 10mg (against 5G)
Alternatively CDS/CDL and zeolite
Dr. Zelenko’s Protocol contains Ivermectin, Hydroxychloroquine (HCQ), Zinc, Vitamin D3, and Quercetin.
 Posted in
Posted in  Tags:
Tags: 













