 RSS Feed
RSS Feed













 August 5th, 2020
August 5th, 2020  Awake Goy
Awake Goy Dr Robert O Young DSc, PhD, Naturopathic Practitioner
What Do Viruses Like HIV & Corona Have In Common With Exosomes?
Jun 5 2020
Authors: Robert O. Young CPC, MSc, DSc, PhD, Naturopathic Practitioner
Galina Migalko MD, NMD
Dr. James Hildreth PhD MD, proposed that “the virus is fully an exosome in every sense of the word.” [1]

Abstract
There is only one sickness, one disease and one treatment. The one sickness and one disease is the over-acidification of the blood and then interstitial fluids due to an inverted way of living, eating, drinking, breathing, thinking, feeling and believing. There are six major contributing factors that lead to the declining acidic pH of the body fluids. As the pH of the body fluids become compensated by these six contributing factors and the body cell membranes and genetic material begin to degenerate the cells release exosomes as a defense to activate and support the lymphocytes to release oxygen species or antioxidants to reduce the acidic loads stored in the interstitial fluids of the Interstitium. The one treatment is to support the immune system with increased amounts of reduced oxygen (O-) and reduced hydrogen (H-) to restore the alkaline design of the body fluids, open up the channels of elimination in order to remove dietary, metabolic, respiratory and environmental toxic acidic waste held in the interstial fluids of the Interstitium and thus restoring health, energy and vitality to the body.

Introduction
What Are Exosomes?

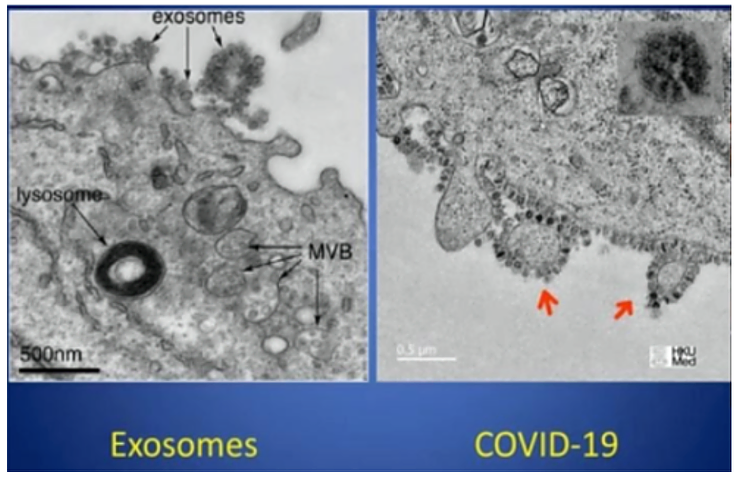
Exosomes are membrane bound extracellular vesicles (EVs) that are produced in the endosomal compartment of most eukaryotic cells.[2][3][4] The multivesicular body (MVB) is an endosome defined by intraluminal vesicles (ILVs) that bud inward into the endosomal lumen. If the MVB fuses with the cell surface (the plasma membrane), these ILVs are released as exosomes. In multicellular organisms, exosomes and other EVs are present in cells that make up tissues and can also be found in biological fluids including intracellular fluids, intravascular fluids, interstitial fluids, urine, and cerebrospinal fluid. They are also released in vitro by cultured cells into their growth medium.[5][6][7][8]
Since the size of exosomes is limited by that of the parent MVB, exosomes are generally thought to be smaller than most other EVs, from about 30 to 150 nanometres (nm) in diameter: around the same size as many lipoproteins but much smaller than cells.[5] Compared with EVs in general, it is becoming more clear that exosomes do have unique characteristics or functions and can be separated or distinguished effectively from other EVs.[2] EVs including exosomes carry markers of cells of origin and have specialized functions in physiological processes, from coagulation and intercellular signaling to acidic waste management of the intravascular and interstitial fluids of the Interstitium – the largest organ of the human body.[5]
Are Exosomes Viruses?
There is NO scientific evidence from ANY research (published or otherwise) from ANY scientist or group of scientists any where in the World validating the existence of the so-called invisible so-called virus or that exosomes have been proven to be the virus.[29]
Exosomes are created endogenously by the cells, even the red blood cells as a means of mediating or buffering metabolic, environmental, dietary and/or respiratory acidic waste in order to maintain the delicate pH balance of the intravascular fluids, the interstitial fluids and the intracellular fluids of the body cells at 7.365.[9][31]
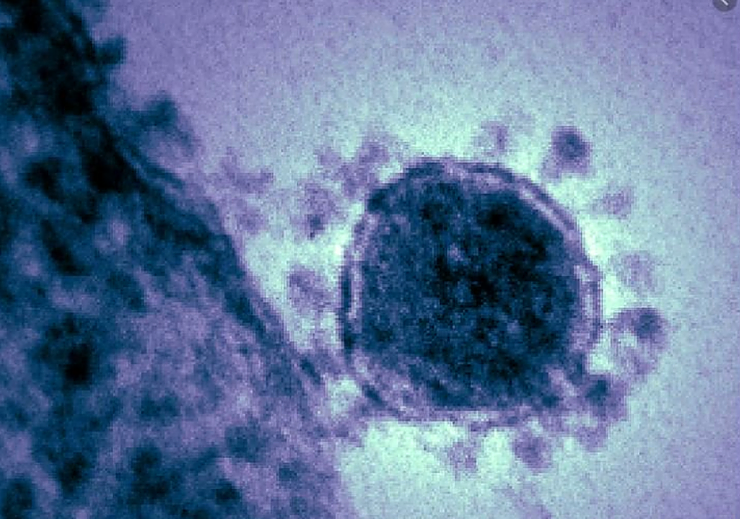
Exosomes and the so-called Corona virus or COVOD-2 and 19 also referred to as the SARS virus are identical in appearance and size and have the same ACE-2 receptor sites, containing the same RNA found in the interstitial fluids of the Interstitium surrounding the cells of the bronchoalveolar. The exosome or the so-called Corona virus is created endogenously and is NOT transmittable or contagious unless transmitted by injection from the isolated exosome(s) of one person or animal to another person.

Endogenously Created Exosomes Protect the Cells
Are COVID-19 and HIV Exosomes?
Based upon electron microscopy the so-called COVID-19 virus and the the so-called HIV virus are 100 nm in diameter and appear identical in structure to the exosome.


Budding of HIV or Exosomes Out of the Plasma Membrane
On January 18th, of 2020, three scientists published a scientific paper describing the protective purpose of exosomes, entitled, “Exosome-Mediated Transfer of ACE2 (Angiotensin-Converting Enzyme 2) from Endothelial Progenitor Cells Promotes Survival and Function of Endothelial Cell.”[9]

Research on Exosomes and Their Support of the Lymphocytes (Immune System) in Reducing Cancer-causing Acidic Waste
Exosomes from red blood cells contain the transferrin receptor which is absent in mature erythrocytes. Dendritic cell-derived exosomes express MHC I, MHC II, and costimulatory molecules and have been proven to be able to induce and enhance antigen-specific T-cell responses in vivo in reducing metabolic, dietary, environmental and respiratory acidic waste deposited into the interstitial fluids of the Interstitium.[10]

What Is the Relationship Between Exosomes and COVID-19
They both contain the ACE2, or angiotensin converting enzyme-2 receptor and visually, using an electron microscope measure the same size. The exosomes or should we say the COVID-19, ACE2 receptor chops up two forms of a protein called angiotensin to keep blood pressure stable by protecting cell membranes from cellular breakdown from metabolic, dietary, environmental and respiratory acidic waste.[9]
So What is Causing the Symptoms of COVID-19 and the Release of Exosomes into the Extracellular Fluid Matrix?
It has come down to a four letter word – ACID! So where is the ACID or toxics coming from?
The seven major contributing factors that cause cellular breakdown and the release of exosomes into the extracellular matrix are as follows:

1. Electro-magnetic pulsating frequencies ranging from 1GHz to 600GHz.[11][12][13]

Computer Board and COV -19 Chip Found in All 5G Cells
2. Carbon Dioxide and Monoxide Poisoning.[14][15][16][17][18][19]
3. Pathological blood coagulation leading to hypoxia, interstitial fluid lung disease, and then sepsis.[20]
4. Glyphosate Acid Poisoning from non-organic fruit and vegetables.[21][22]
5. Lactic Acid Poisoning from diet and metabolism.[21]22]
6. Uric, Nitric, Sulphuric and Phosphoric Acid Poisoning from eating the flesh and blood of animals.[21][22]
7. Genetically Modified Organisms in our food supply and vaccines.[21][22] [Please see the comparisons of flu vaccine frequency in older people with Covid-19 mortality, using figures fromVaccines Today EU and Worldometer (13 May 2020):[23]

Among countries omitted in the EU data was Belgium, which has the highest Covid-19 mortality rate in the world, at 763 per million. While specific data for older people were not available on the official Belgian statistics website, flu vaccination coverage of the overall population is relatively high.
Electron Micrograph of the Exosome Associated with H1N1 So-Called Swine Flu Virus
Globally the highest uptake of the flu vaccine by seniors in 2018-2019 was in South Korea, at 83%. Third (after the UK) was the USA with 68%, and fourth was New Zealand with 67%.
Vaccines may be a contributing factor to other so-called viral conditions . As reported in , whooping cough outbreaks have infected vaccinated as well as unvaccinated people.[24][25] Mandating of the chickenpox vaccine in the USA appears to have weakened the immunity gained from the naturally-acquired disease; a review by Goldman and King inVaccine journal showed increasing incidence of shingles.[26] Studies have indicated that people receiving the flu vaccine in one year were more likely to contract the H1N1 strain of exosomes in the following year.[27][28]

Despite some contrary cases, it is significant that the countries with highest death rates (Belgium, Spain, Italy, UK, France, Netherlands, Sweden, Ireland and USA) had all vaccinated at least half of their elderly population against flu. Denmark and Germany, with lower use of the flu vaccine, have considerably lower Covid-19 mortality. These patterns override interventions to curtail Covid-19: Sweden and Ireland have similar mortality but the former remained open for business while the other imposed strict lockdown.
Methodology
In order to obtain the micrographs of exosomes or so-called viruses RT electronmicroscopy was used in addition to phase and dark field microscopy on the intravascular and interstitial fluids of the extracellular fluid matrix. We also used a unique patent-pending electron device for measuring the biochemistry, including the pH for analytical comparisons of the intracellular fluid matrix which include the intravascular and interstitial fluids of the Interstitium, the largest organ of the human body. By measuring all the body fluids for their biochemistry it was clear that patients who tested positive for HIV and Cornavirus where in decompensated acidosis of the interstitial fluids, including the interstitial fluids of the lungs.[20][31]
Conclusion
Exosomes are the so-called viruses since viruses have never been identified, isolated, purified, and cultured based upon the scientific method called Koch’s Postulates.[34] Exosomes are released endogenously from the body cells to assist in activating the immune response due to decompensated acidosis of the interstitial fluids of the Interstitium. Decompensated acidosis of the body fluids causes cell membrane degeneration and genetic mutation leading to all sicknesses and diseases. There are at least seven major contributing toxic factors that cause the increased levels of acidity in the body fluids leading to a significant decline in the alkaline design of the major body fluids (interstitial fluids of the Interstitium organ and the intravascular fludis) from their ideal pH of 7.365 to an unhealthy pH of 7.265 to 7.165. The seven major contributing acidic factors that cause all sickness and disease are:
1) pulsating electro-magnetic fields from satellites, cell phones, computers, cell towers, WiFi, electric cars, TV’s, etc.,
2) carbon dioxide and carbon monoxide poisoning from air-pollution,
3) pathological blood coagulation leading to hypoxia, interstitial lung disease and sepsis,
4) glyphosate poisoning from food, water and vaccines,
5) lactic acid poisoning from diet and metabolism,
6) uric, nitric, sulphuric and phosphoric acid poisoning from indigestion of eggs, fish, beef, chicken and pork, and finally,
7) the introduction of genetically modified organisms and aluminum oxide poisoning from vaccines and chem trails.[27-31]
[Truth11.com note: There is another article below these references, please read on!]
References
[1] https://rupress.org/…/6/9…/33690/When-is-a-virus-an-exosome…
[2] Théry C, Witwer KW, Aikawa E, Alcaraz MJ, Anderson JD, Andriantsitohaina R, et al. (2018). “Minimal information for studies of extracellular vesicles 2018 (MISEV2018): a position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines”. Journal of Extracellular Vesicles. 7 (1): 1535750. doi:10.1080/20013078.2018.1535750. PMC 6322352. PMID 30637094.
[3] Yáñez-Mó M, Siljander PR, Andreu Z, Zavec AB, Borràs FE, Buzas EI, Buzas K, et al. (2015). “Biological properties of extracellular vesicles and their physiological functions”. Journal of Extracellular Vesicles. 4: 27066. doi:10.3402/jev.v4.27066. PMC 4433489. PMID 25979354.
[4] van Niel G, D’Angelo G, Raposo G (April 2018). “Shedding light on the cell biology of extracellular vesicles”. Nature Reviews. Molecular Cell Biology. 19 (4): 213–228. doi:10.1038/nrm.2017.125. PMID 29339798.
[5] van der Pol E, Böing AN, Harrison P, Sturk A, Nieuwland R (July 2012). “Classification, functions, and clinical relevance of extracellular vesicles”. Pharmacological Reviews. 64 (3): 676–705. doi:10.1124/pr.112.005983. PMID 22722893.
[6] Keller S, Sanderson MP, Stoeck A, Altevogt P (November 2006). “Exosomes: from biogenesis and secretion to biological function”. Immunology Letters. 107 (2): 102–8. doi:10.1016/j.imlet.2006.09.005. PMID 17067686.
[7] Spaull R, McPherson B, Gialeli A, Clayton A, Uney J, Heep A, Cordero-Llana Ó (April 2019). “Exosomes populate the cerebrospinal fluid of preterm infants with post-haemorrhagic hydrocephalus”. International Journal of Developmental Neuroscience. 73: 59–65. doi:10.1016/j.ijdevneu.2019.01.004. PMID 30639393.
[8] Dhondt B, Van Deun J, Vermaerke S, de Marco A, Lumen N, De Wever O, Hendrix A (June 2018). “Urinary extracellular vesicle biomarkers in urological cancers: From discovery towards clinical implementation”. The International Journal of Biochemistry & Cell Biology. 99: 236–256. doi:10.1016/j.biocel.2018.04.009. PMID 29654900.
[9] Wang J, Chen S, Bihl J, “Exosome-Mediated Transfer of ACE2 (Angiotensin-Converting Enzyme 2) from Endothelial Progenitor Cells Promotes Survival and Function.” Oxid Med Cell Longev, 2020 Jan 18;2020:4213541. doi: 10.1155/2020/4213541
[10] Mignot G, Roux S, Thery C, Ségura E, Zitvogel L (2006). “Prospects for exosomes in immunotherapy of cancer”. Journal of Cellular and Molecular Medicine. 10 (2): 376–88. doi:10.1111/j.1582-4934.2006.tb00406.x. PMC 3933128. PMID 16796806.
[11] Rubik, B. Bioelectromagnetic Medicine. Administrative Radiology Journal XVI(8), August 1997, 38-46.
[12] Young, R.O., “The Effects of ElectroMagnetic Frequencies (EMF) on the Blood and Biological Terrain.” https://www.drrobertyoung.com/…/the-effects-electromagnet-f…
[13] Young, R.O., “Adverse Health Effects of 5G Mobile Networking Technology Under Real-Life Conditions.” April 19th, 2020. https://www.drrobertyoung.com/…/adverse-health-effects-of-5…
[14] NOAA. (2016). In a high carbon dioxide world, dangerous waters ahead. (accessed on August 6, 2019)
[15] NOAA. (2018). What is Ocean Acidification? (accessed on August 6, 2019)
[16] National Geographic. (2017). Ocean Acidification. (accessed on August 6, 2019)
[17] NOAA. (2010). Ocean Acidification, Today and in the Future. (accessed on August 6, 2019)
[18] Young, R.O., Young, S.R, “The pH Miracle Revised and Updated.” Hachett Publishing, 2010.
[19] Young, R.O., Are the Interstitial Fluids Raining Acid on YOUR Lung Cells? (December 17th, 2019)
[20] Young, R.O., Migalko, G., “Interstitial Fluid Lung Disease (IFLD) of the Interstitium Organ the Cause and Self-Care to a Self-Cure for Lung Disease”. International Journal of Cancer Research & Therapy, https://bit.ly/2xD8VBP, January 20, 2020.
[21] Young, R.O., “Sick and Tired.” https://www.phmiracleproducts.com/…/books-audio-video/produ…
[22] Young, R.O., Young, S.R. “The pH Miracle Revised and Updated.” Grand Central Publishing, NY, NY, 2010. https://www.phmiracleproducts.com/…/the-ph-miracle-revised-
[23] Vaccines Today, EUandWorldometer (13 May 2020).
[24] Althouse, B.M., Scarpino, S.V. Asymptomatic transmission and the resurgence ofBordetella pertussis.BMC Med 13,146 (2015). https://doi.org/10.1186/s12916-015-0382-8…
[25] Zhang Q, Yin Z, Li Y, Luo H, Shao Z, Gao Y, et al.Prevalence of asymptomatic Bordetella pertussis and Bordetella parapertussis infections among school children in China as determined by pooled real-time PCR: A cross-sectional study. Scand J Infect Dis. 2014; 46:280–7.
[26] Goldman GS, King PG, “Review of the United States universal varicella vaccination program: Herpes zoster incidence rates, cost-effectiveness, and vaccine efficacy based primarily on the Antelope Valley Varicella Active Surveillance Project data.” Vaccine, 2013 Mar 25;31(13):1680-94. doi: 10.1016/j.vaccine.2012.05.050. Epub 2012 Jun 1.
[27] Cécile Viboud, Lone Simonsen, “Does Seasonal Influenza Vaccination Increase the Risk of Illness with the 2009 A/H1N1 Pandemic Virus?” PLoS Med. 2010 Apr; 7(4): e1000259.
[28] Belongia EA, Skowronski DM, McLean HQ, Chambers C, Sundaram ME, De Serres G, “Repeated annual influenza vaccination and vaccine effectiveness: review of evidence.” Expert Rev Vaccines. 2017 Jul;16(7):1-14. doi: 10.1080/14760584.2017.1334554. Epub 2017 Jun 9.
[29] Young, R.O.,”Chlorine Dioxide (CLO2) As a Non-Toxic Antimicrobial Agent for Virus, Bacteria and Yeast (Candids Albicans),” Hikari Omni Media, August 2nd, 2016. https://www.phmiracleproducts.com/…/chlorine-dioxide-clo2-b…
[30] Young, R.O., Migalko, G., “Alkalizing Nutritional Therapy in the Prevention and Treatment of any Cancerous Condition.” Hikari Omni Media, August 1st, 2016. https://www.phmiracleproducts.com/…/alkalizing-nutritional-…
[31] Young, R.O., “Second Thoughts about Viruses, Vaccines, and the HIV/AIDS Hypothesis,” Hikari Omni Media, August 2nd, 2016. https://www.phmiracleproducts.com/…/second-thoughts-about-v…
[32] Young, R.O., “The Possible Cause of Polio, Post-Polio, CNS, PVIPD, Legionnaires, AIDS and the Cancer Epidemic – Mass Acidic Chemical Poisoning?” Hikari Omni Media, October 19, 2016. www.phmiracleproducts.com
[33] Young, R.O., “Pathological Blood Coagulation and the Mycotoxic Oxidative Stress Test (MOST)”: https://medcraveonline.com/IJVV/IJVV-02-00048, September 20, 2016.
[34] Tabrah, F.L., “Koch’s Postulates, Carinvorous Cows, and Tuberculosis Today.” Hawaii Med J. 2011; Jul;70(7): 144-148.
Artilce 2.
The Genesis of Severe Acute Respiratory (Syndrome) Disease or SARS (Coronavirus – COVID – 2 and 19)
Updated: May 24
Authors: Robert O Young DSc. PhD. and Dr. Galina Migalko MD, NMD
16390 Dia del Sol, Valley Center, California 92082
Interstitial Fluid Lung Disease (IFLD) of the Interstitium Organ The Cause and Self-Care to a Self-Cure for Lung Disease
Abstract
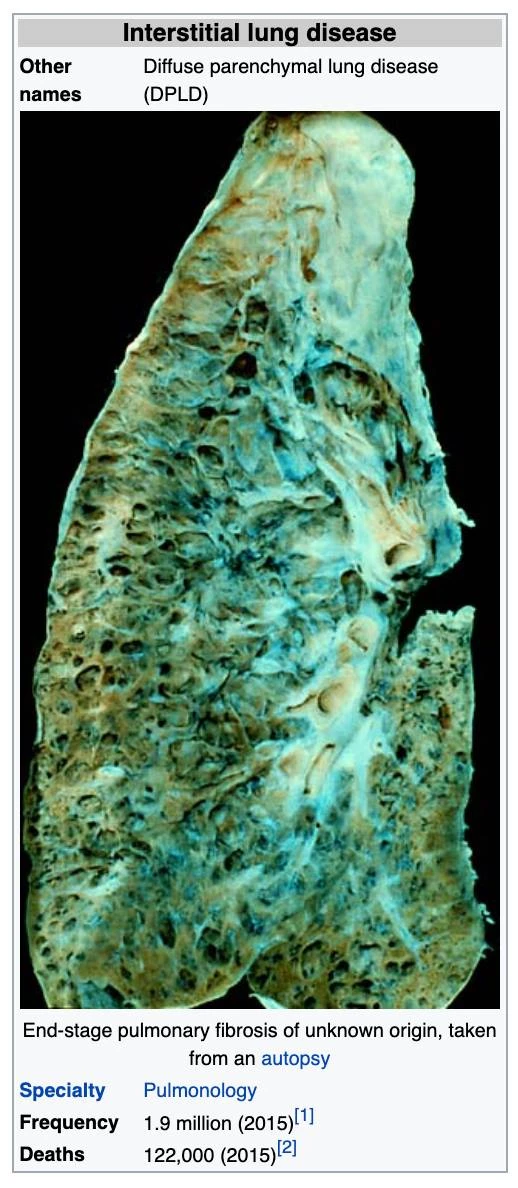
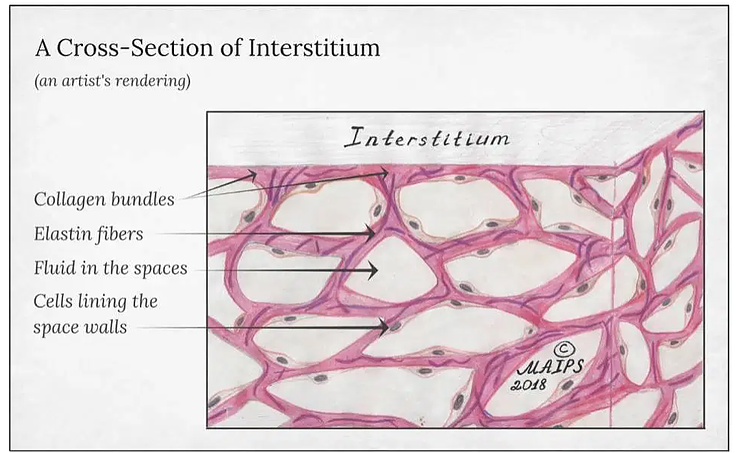
Interstitial lung disease (IFLD), or diffuse parenchymal lung disease (DPLD),[3] is a group of lung diseases affecting the Interstitium (the interstitial fluids or space around the alveoli (air sacs of the lungs).[4]
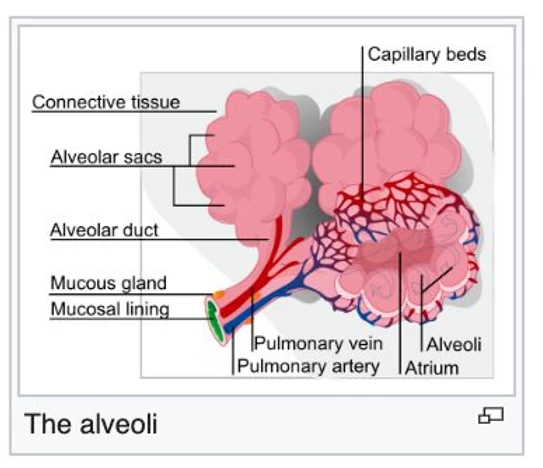
It concerns alveolar epithelium, pulmonary capillary endothelium, basement membrane, and perivascular and perilymphatic tissues. It occurs when metabolic, dietary, respiratory and environmental acids injure the lung tissues that triggers an abnormal healing response. Ordinarily, the body generates just the right amount of tissue to repair acid damage, but in interstitial lung disease, the repair process goes awry because of the acidic pH (ideal healing takes place at a pH of 7.365)[5]) of the interstitial fluids that effects the normal healing of the tissue around the air sacs (alveoli) and therefore becomes scarred anthickened.

Micrograph of usual interstitial pneumonia (UIP). UIP is the most common pattern of interstitial pneumonia (a type of interstitial lung disease) and usually represents pulmonary fibrosis caused by decompensated acidosis of the interstitial fluids of the largest organ of the human body – the Interstitium. H&E stain. Autopsy specimen.
This makes it more difficult for oxygen to pass into the bloodstream. The term ILD is used to distinguish these diseases from obstructive airways diseases but the cause of all lung disease is due to decompensated acidosis of the interstitial fluids (pH is below 7.2) that is systemic although affecting the weakest area of the lungs. These weaknesses can be attributed to lifestyle and dietary choices
There are specific types of interstitial lung disease in children. The acronym chILD is used for this group of diseases and is derived from the English name, Children’s Interstitial Lung Diseases – chILD.[6]
Prolonged interstitial lung disease may result in pulmonary fibrosis, but this is not always the case. Pulmonary fibrosis is specifically caused by the increase of acids in the interstitial fluids of the lung due to an inverted way of living, eating, drinking, breathing, thinking, feeling and believing. Interstitial lung disease of the Interstitium is associated with typical findings both radiographic (basal and pleural-based fibrosis with honeycombing) and pathologic (temporally and spatially heterogeneous fibrosis, histopathologic honeycombing, and fibroblastic foci).
Our findings using advanced technologies with non-invasive, non-radioactive 3D Bio-Electro Scanning of the Interstitial fluids of the largest organ of the body, the Interstitium to determine a complete chemistry, including pH. This testing has shown in all cases of interstitial fluid lung disease, including viral diseases, and malignancies with 98 percent accuracy for decompensated metabolic acidosis, of the IFLD, high levels of lactic acid and high levels of calcium. Since the interstitial fluids pass through every organ, gland and tissues we now have a complete picture of the functionality and chemistry of every organ, every gland and every tissue, including all bones and muscles.
Introduction
In 2015, interstitial lung disease, together with pulmonary sarcoidosis, affected 1.9 million people.[1] They resulted in 122,000 deaths.[2] and can be reversed with a specific alkaline lifestyle, including a specific alkaline diet, alkalizing exercise, alkalizing rectal infusion, alkalizing nebulization with specific water-based anti-oxidants, breathing techniques, transcendental meditation, specific alkalizing support with alkaline water, vitamins, minerals, herbal and the 12 tissue salt supplements and other techniques discovered by Robert O. Young PhD and Galina Migalko MD, NMD. [7]
The following are the names or specific symptoms given to Interstitial Lung Disease. The cause of ALL of these symptoms are the result of an acidic lifestyle, as listed below. [7]
The Symptoms of Interstitial Fluid Lung Disease (IFLD) of the Interstitium
The alveoli
Micrograph of usual interstitial pneumonia (UIP). UIP is the most common pattern of interstitial pneumonia (a type of interstitial lung disease) and usually represents pulmonary fibrosis. H&E stain. Autopsy specimen.
ILD may be classified according to the symptoms of decompensated acidosis of the interstitial fluids of the lung.[8]
Methodology Classification by IFLD Symptoms is as follows:
Inhaled substances Inorganic:
Silicosis Asbestosis Berylliosis Industrial printing chemicals (eg. carbon black, ink mist)
Inhaled substances Organic:
Hypersensitivity pneumonitis
Drug-induced
Antibiotics Chemotherapeutic drugs
Antiarrhythmic agents
Connective tissue and Autoimmune diseases
Rheumatoid arthritis Systemic lupus erythematosus Systemic sclerosis Polymyositis Dermatomyositis Infection Outfection Atypical pneumonia Pneumocystis pneumonia (PCP)
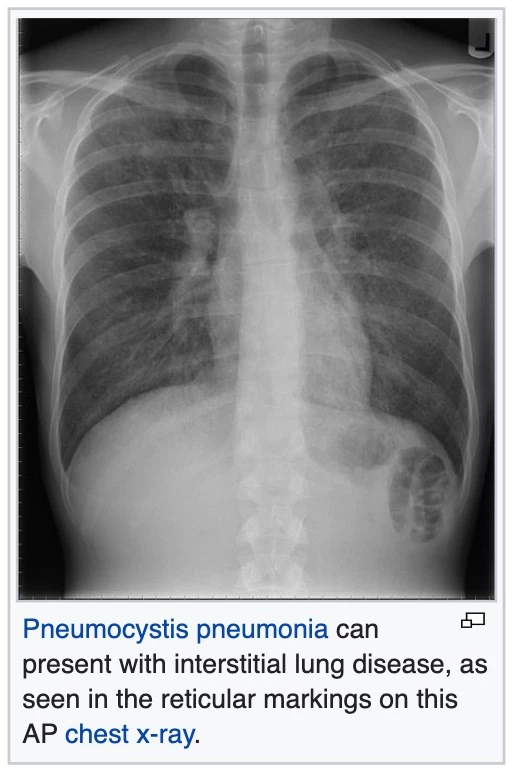
Tuberculosis Chlamydia trachomatis Respiratory Syncytial Virus Sarcoidosis Pulmonary fibrosis

Hamman-Rich syndrome Antisynthetase syndrome
Malignancy
Lymphangitic carcinomatosis
Predominately in children
Diffuse developmental disorders Growth abnormalities deficient alveolarization
Infant conditions of undefined cause
ILD related to alveolar surfactant region
Methodology
Diagnosis of Interstitial Lung Disease and All Other Associated Conditions
Investigation is tailored towards the symptoms and signs. A proper and detailed history looking for the occupational exposures, and for signs of conditions listed above is the first important part of the workup in patients with Interstitial Lung Disease. Pulmonary function tests usually show a restrictive defect with decreased diffusion capacity (DLCO). [9]

Testing the urine pH, saliva pH, stomach pH, blood pH, and interstitial fluids pH with a complete chemistry are all non-invasive medical tests unique to our 75 years of combined research to discover the cause of ALL sickness and disease, including ones which are idiopathic. The non-invasive medical diagnostics for ITL is called the 3D Full Body Functionality and Interstitial Fluid Testing (FBBES). [10]
New Methods for Whole Body Non-Invasive Diagnostic Testing of the Blood, Interstitial Fluids and Intracellular Fluids
Using 3-D Full Body Bio-Electro Scanning (FBBES), Full Body Thermography (FBT), Full Body Ultrasound (FBU), Live Blood Analysis (LBA) and Dried Blood Analysis (DBA) to Determine the Best Possible Strategy for Preventing and/or Reversing Any Sickness or Disease Condition and to Monitor Effective Treatment Progress [10].
In modern day conventional medicine, surgeons biopsy the lymph nodes and lung tissue to determine how lung disease, including malignancy is spreading to provide staging [11]. Lymphocytes, a type of white blood cell that is found in these lymph nodes which are catch-basins for acidic waste and malignant cells are responsible for breaking-down and removing cellular acidic waste and genetically mutated cells. Impaired lymphocytes and lymph nodes are at least one major factor in the many areas we test for (as described below) physiologically using functionality testing (FBBES) (as described below). The lymphatic system, the lymph nodes and the lymphocytes themselves must be functional in order to prevent and reverse any disease condition, including Interstitial Lung Disease (ILD).
Using electrodes attached to the head, hands, and feet, the functionality of the lymphatic system, circulatory system, muscular system, skeletal system, endocrine system, neurological system, reproductive system, vascular system, digestive system, and respiratory system can be non-invasively analyzed.
Interstitial chemistry, interstitial pH to determine decompensated acidosis, and the electro-conductivity of the cells to determine the state of health of all organs, glands, and tissues in the prevention and reversal of any disease condition, including ILD.
This FBBES also accounts for nutritional deficiencies and metabolic alkalosis or acidosis by measuring the interstitial chemistry, interstitial pH, and the electro-conductivity if the cells of the body. Measuring the pH of the interstitial fluids is more revealing as it pertains to the pH and chemistry than measuring the blood fluids for ILD condition since the blood is always trying to maintain its delicate alkaline pH of 7.365 and will not vary much. Based upon our research we have determined that ILD and all of its many symptoms are expressed as a compromised acidic environment of the interstitial fluids which may negatively affect the state of health of all body cells which make up the organs, glands and tissues, including the lung cells. [12].
It is significantly more important to measure interstitial and intracellular fluids than blood fluids in order to obtain a correct chemistry and pH when making nutritional recommendations in the prevention and treatment of ILD and any malignancy [13].
The following are quantitative measurements in healthy patients, without ILD or malignancy of the lung, comparing blood fluids with intracellular and interstitial fluids of the body compartments as a benchmark to determine deficiencies in alkalizing minerals, protein, and whether or not the patient is in decompensated acidosis of the interstitial fluids, a pre-malignancy, or malignant condition (Note: all ILD and cancer patients are in decompensated interstitial acidosis, low in interstitial sodium and high in interstitial calcium and potassium): [13]
1) Sodium: Na+ mEq/l Venous blood: 130, Arterial blood: 137, Capillary blood: 135, Intracellular fluid: 10 and Interstitial fluid: 135
2) Potassium: K+ mEq/l Venous blood: 3.2, Arterial blood: 3.5, Capillary blood: 4, Intracellular fluid: 140 and Interstitial fluid: 3.17
3) Calcium: Ca++ mEq/l Venous blood: 2.5, Arterial blood: 2.2, Capillary blood: 2.3, Intracellular fluid: 0.0001 and Interstitial fluid: 1.55
4) Magnesium: Mg mEq/l Venous blood: 0.64, Arterial blood: 0.62, Capillary blood: 0.60, Intracellular fluid: 58 and Interstitial fluid: 0.50
5) Chloride: Cl- mEq/l Venous blood: 104, Arterial blood: 101, Capillary blood: 103, Intracellular fluid: 4 and Interstitial fluid: 106
6) Bicarbonate: HCO3 mEq/l Venous blood: 22, Arterial blood: 24, Capillary blood: 23, Intracellular fluid: 10 and Interstitial fluid: 24
7) Phosphorus: P mE/l Venous blood: 2.5, Arterial blood: 2.3, Capillary blood: 2, Intracellular fluid: 75 and Interstitial fluid: 0.70
8) Sulfate: SO4 mEq/l Venous blood: 0.8, Arterial blood: 0.6, Capillary blood: 0.5, Intracellular fluid: 2 and Interstitial fluid: 0
9) Glycemia mg/dl Venous blood: 1, Arterial blood: 1, Capillary blood: 1.01, Intracellular fluid: 0.20 and Interstitial fluid: 0.90
10) Cholesterol mg/dl Venous blood: 0.66, Arterial blood: 0.630, Capillary blood: 0.676, Intracellular fluid: 0.2 and Interstitial fluid: 0.188
11) Partial Pressure of Oxygen or PO2 mmHg Venous blood: 80, Arterial blood: 90, Capillary blood: 89, Intracellular fluid: 20 and Interstitial fluid: 87.2
12) Carbon Dioxide Or PCO2 Venous blood: 46, Arterial blood: 40, Capillary blood: 42, Intracellular fluid: 50 and Interstitial fluid: 46
13) pH or potential of hydrogen Venous blood: 7.36, Arterial blood: 7.4, Capillary blood: 7.38, Intracellular fluid: 7.2 and Interstitial fluid: 7.36
14) Protein g/dl Venous blood: 72, Arterial blood: 74, Capillary blood: 73.7, Intracellular fluid: 68 and interstitial fluid: 20.6
The following are quantitative measurements in healthy patients, without IFLD or malignancy of the lung, comparing blood fluids with intracellular and interstitial fluids of the body compartments as a benchmark to determine deficiencies in alkalizing minerals, protein, and whether or not the patient is in decompensated acidosis of the interstitial fluids, a pre-malignancy, or malignant condition (Note: all ILD and cancer patients are in decompensated interstitial acidosis, low in interstitial sodium and high in interstitial calcium and potassium): [13]
Results
Using non-invasive 3D-FBBES for determining the chemistry of the interstitial fluids of the whole body, including the lungs is not only a test for determining decompensated acidosis or compensated alkalosis (a pre-condition of IFLD) of the ALL interstitial fluids of the body, including the lungs, but is an effective way to determine efficacy of any medical or natural alkalizing therapy in prevention and treatment of ANY sickness or disease. The results of the using 3D-GBBES combined with conventional medical blood tests and/or the Non-Invasive Blood Tests [NIBT] covering over 170 parameters of the blood, including blood counts, chemistry, pH of the blood, stomach and most important quantifying acid loads, such as lactic acid with a 98 percent accuracy for determining pre-interstitial-fluid lung disease and IFLD and its many symptomologies as listed above.
References
1. GBD 2015 Disease and Injury Incidence and Prevalence, Collaborators. (8 October 2016). “Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015”. Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282. 2. GBD 2015 Mortality and Causes of Death, Collaborators. (8 October 2016). “Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015”. Lancet. 388 (10053): 1459–1544. doi:10.1016/S0140-6736(16)31012-1. PMC 5388903. PMID 27733281. 3. King TE (August 2005). “Clinical advances in the diagnosis and therapy of the interstitial lung diseases”. American Journal of Respiratory and Critical Care Medicine. 172 (3): 268–79. doi:10.1164/rccm.200503-483OE. PMID 15879420. 4. “Frequently Asked Questions About Interstitial Lung Disease”. University of Chicago Medical Center.
5. Young RO, Migalko G (2015) Alkalizing Nutritional Therapy in the Prevention and Reversal of any Cancerous Condition. Int J Complement Alt Med 2(1): 00046. DOI: 10.15406/ijcam.2015.02.00046 6. Bush A, Cunningham S, de Blic J, Barbato A, Clement A, Epaud R, Hengst M, Kiper N, Nicholson AG, Wetzke M, Snijders D, Schwerk N, Griese M (November 2015). “European protocols for the diagnosis and initial treatment of interstitial lung disease in children”. review. Thorax. 70 (11): 1078–84. doi:10.1136/thoraxjnl-2015-207349. PMID 26135832.
7. Young Robert, Young Shelley (2010) The pH Miracle. Balance Your Diet, Reclaim Your Health. Hachett Publishing, Haryana, India. 8. Bourke SJ (August 2006). “Interstitial lung disease: progress and problems”. Postgraduate Medical Journal. 82 (970): 494–9. doi:10.1136/pgmj.2006.046417. PMC 2585700. PMID 16891438. 9. Ryu JH, Olson EJ, Midthun DE, Swensen SJ (November 2002). “Diagnostic approach to the patient with diffuse lung disease”. Mayo Clinic Proceedings. 77 (11): 1221–7, quiz 1227. doi:10.4065/77.11.1221. PMID 12440558. 10. Galina Migalko, Universal Medical Imaging Group, Valley Village, California, USA. www.universalmedicalimaging.com
11. Ronald G.CrystalM.D., James E.GadekM.D., Victor J.FerransM.D., Jack D.FulmerM.D., Bruce R.LineM.D., Gary W.HunninghakeM.D, “Review Interstitial lung disease: Current concepts of pathogenesis, staging and therapy”. The American Journal of Medicine
Volume 70, Issue 3, March 1981, Pages 542-568.
12. Rose BD (2001) Post TW. Clinical Physiology of Acid-Base and Electrolyte Disorders, (5th edn), McGraw-Hill, New York. p. 347.
13. Young RO, Migalko G (2015) Alkalizing Nutritional Therapy in the Prevention and Reversal of any Cancerous Condition. Int J Complement Alt Med 2(1): 00046. DOI: 10.15406/ijcam.2015.02.00046.
 Posted in
Posted in  Tags:
Tags: 
















