 RSS Feed
RSS Feed















 December 17th, 2022
December 17th, 2022  Awake Goy
Awake Goy Germany Has Provided The Means To Quantify The Human Cost Of The Experimental Vaccination Program

Dec 12 2022
Most sane people believe that the burden of proving safety should lie on the party conducting a questionable action, rather than their victim. For example, if a criminal shot someone, the prosecution would not be required to prove that the victim’s sudden death after the gunshot wound was not just a spontaneous coincidence, a result of extreme stress from the situation, or due to a pre-existing medical condition.
Unfortunately, the pharmaceutical industry has been able to establish a special type of privilege within the legal system and has made it very difficult to demonstrate that vaccines (along with many other pharmaceuticals) can ever be at fault for anything. Because of this, we recently had a flood of experimental vaccines mandated upon the population, which were never tested for safety (despite many serious concerns with their design), whose (likely fraudulent) clinical trial data was never made accessible to the public. We then had, as far as I know, the most aggressive propaganda campaign in history, and I watched the majority of my colleagues lose the ability to recognize any problems related to the vaccines. Instead, they developed an almost surreal religious devotion to the coming salvation (the vaccines becoming available).
Once the vaccines entered the market, a variety of red flags began going off indicating that these vaccines were killing people, and rather than address these concerns, the government—in concert with the media—chose to deny any of this was occurring. Instead they mandated the vaccines upon the entire population. I was understandably worried that the vaccines would cause problems and tried to do my part to head this off in 2020, but I did not expect anything on the scale of what we have encountered since then.
I personally became involved in all of this because soon after the vaccines entered the market, I began to have many friends and patients reach out to ask me if the vaccine could kill, because someone they knew had had a tragic sudden death after vaccination. Once the magnitude of the problem dawned on me, I realized that even though my available options were limited, I could at least do my best to document each case sent my way so that someone would bear witness to what had happened. Otherwise, the dead had no voice. Other than knowing I had a duty to compile this list, I was not sure what to do with it. Later after someone kindly helped launch this Substack, I decided to post it, it ended up being seen by a lot of people…and that is how I ended up writing here.
Because of how long it took to verify each case, I realized that I had to end it a year in (at which point I knew of 45 individuals who had either critical or fatal injuries of a similar nature in close proximity to vaccination). Since that time, I still continue to hear reports I periodically document and discuss.
For example, a good friend is a nurse in a cardiac unit and has told me many of the patients she sees now with heart failure are much younger than they were a few years ago. I previously advised her against getting the vaccine due to her history of rheumatic fever (a condition where the immune system attacks and damages part of the heart). This was because I had noticed both COVID-19 and especially its vaccine seemed to cause inflammatory flares at previous sites of injuries or inflammation (Lyme is also known for doing this). The vaccine also has a remarkably high rate of exacerbating pre-existing autoimmune conditions—such as the 24.2% rate found in a recent Israeli survey which is comparable to what a few colleagues have observed, and I suspect exacerbation of preexisting inflammation in the circulatory system, like what this study of 566 patients found, is a key mechanism behind vaccine deaths.
A month ago, that same friend I had advised against vaccinating informed me that she had developed a heart condition from the vaccine, her mother had as well ), and that her sibling’s partner is suffering longterm complication from a stroke that immediately followed a booster.
Looking back on it, the thing I found the most disappointing about my own documentation project was that once it went viral, it should have triggered the drug regulators evaluating the vaccines to take preventative action. Instead, due to the meticulously planned campaign of mass censorship that we all found ourselves in, more red flags than I can count were ignored by the “very rigorous” vaccination surveillance systems that were allegedly ensuring there were no safety issues with these vaccines.
Because of the immense power behind the medical-industrial complex, those debating this program have been stuck fighting an uphill battle. However, despite the immense degree of corruption, withholding of critical data, and censorship, these vaccines are dangerous enough that more and more evidence is nonetheless emerging of their danger, and the public is beginning to recognize it. The previous article that was posted detailed how this appears to be happening:
The Forgotten Side of Medicine
We Now Have A Clear Estimate Of The Rate Of Vaccine Injuries
4 days ago · 396 likes · 397 comments · A Midwestern Doctor
After it was published, I was informed by a reader that possibly the most important dataset over the last two years was released today. For those interested, much of the context for today’s article can be found in the article above.
German Data
One of the depressing realizations one gains from studying the evidence-based literature is discovering how many issues exist within it and how difficult it is to know which data sources can be trusted. One of my favorite authors, Dr. Malcom Kendrick, devoted a book to addressing this subject and shared a pertinent anecdote for today’s events:
“In truth, the figures on vaccine damage are exceedingly difficult to analyse, because causality is very difficult to prove on a case by case basis. However, when it comes to negative findings I always like to go to Germany. It has been demonstrated many times that the Germans are the most likely to report negative findings accurately. Yes I know, terrible racial stereotyping, but a fact is a fact. What do the Germans have to say on the matter?
“Between 1978 and 1993 approx. 13,500 cases of undesired effects resulting from medications for vaccinations was reported to the Paul Ehrlich-Institute (PEI)…the majority was reported by the pharmaceutical industry. In 40% [5,400] of these cases the complications were severe, 10% [1,350] pertained to fatalities on account of effects.”
Additionally, as I learned from Kendrick, since early 2001, the federal infection protection law has mandated that specific severe vaccine injuries be immediately reported directly to the PEI (Germany’s equivalent of the FDA for vaccines and biologics). The German’s list of reportable injuries is much broader than what I have seen acknowledged by many other countries (e.g. those which are possible to receive compensation for within the United States) and includes the previously discussed complications of DPT along with many of the reactions typically associated with the COVID-19 vaccines. However, while that historical trend exists, Germany has not been one of the best countries for reporting COVID vaccine injuries (which I suspect is due to the political direction their government has moved in).

(The above graph illustrates why many of my German friends are not happy with their government)
Because of their tradition of reporting adverse reactions to vaccination, Germans (or at least some of them) have been more resistant to toeing the party line on concealing the dangers of the COVID-19 vaccines than citizens of many other countries (my friends there are enraged by the egregious concealment of critical safety data by the German government). In turn, some of the most critical vaccine data available comes from the German people as many of them have retained their intellectual integrity throughout the pandemic.
For instance, although autopsies should always be conducted on those who died suspiciously after vaccination, due to the global climate of intimidation against conducting any type of research that challenges the COVID vaccine program, it is rarely done. Instead, almost every autopsy has been performed by a few brave pathologists in Germany, and I have tried to detail the pathologist’s work throughout my postings (e.g., see here).
Some of the most important contributions of these autopsies include:
•Demonstrating that there is highly unusual tissue inflammation in those who died after vaccination. Pathologists had not observed this phenomena before the COVID-19 vaccines, and they suspected this inflammation would be fatal.
•Demonstrating that the COVID spike protein could also be found in the tissues of those who died.
•Demonstrating that another key part of the SARS-CoV-2 virus was not present, meaning that the only possible source of the spike protein was the vaccine.
The most definitive study on this subject was recently completed. It examined 35 individuals who died within 20 days of vaccination, and after a lengthy examination excluded 10 who had a potential cause of death other than vaccination. Of the remaining 25, most had causes of death that frequently been linked to vaccination, and of those, 5 were found to have myocarditis potentially linked to the vaccine, and in 3 cases the vaccine was determined to be the definitive cause of their myocarditis and death. These results are very important for convicting the vaccines if it can also be proven that a large number of unexpected deaths are occurring following vaccination.
The Religion of Data
Every group needs to have some type of ideology to unite behind. Presently, one of the fixations within the Western world is on more and more data being the solution to everything. In turn, there are many concerns with this approach (e.g., it dehumanizes people, its “necessity” is used to justify violating citizen’s right to privacy while collecting it and it is being used to build an infrastructure that controls every aspect of our lives).
Although data is often claimed to be our salvation, and I will admit sometimes is quite helpful, in many other cases, it fails abysmally to address our problems. A major reason for this failure is that no one wants to critically analyze data this is gathered if that data suggests we should stop supporting an entrenched financial interest.
I am most aware of this in healthcare, as I know of numerous systems which were designed to analyze electronic medical records and either identify which pharmaceutical worked best for a condition, or if a pharmaceutical (or vaccine) was unsafe. Not surprisingly, all of these systems were never adopted, and the endless data we collect in healthcare (e.g., all the diagnostic coding data which medical insurance providers provide as a condition of reimbursement to healthcare providers) is rarely utilized to improve the public good. However, while prevailing biases frequently produces flawed analyses of data, data itself does not lie and has immense potential to expose dangerous health care practices if people are willing to look at it.
The largest insurance provider in Germany, BKK, provides coverage to approximately 10.9 million Germans. A board member, Andreas Schöfbeck, observed some very concerning signs in their data, and unlike everyone else, had the courage to disclose it in a letter to the German government (e.g. he addressed the PEI), after which, he was dismissed from his position. The BKK dataset (discussed by Jessica Rose) was the one which showed 2.05% of vaccine recipients subsequently sought medical care with a healthcare provider (others estimated it demonstrated 3.5% were struggling with persistent vaccine side effects).
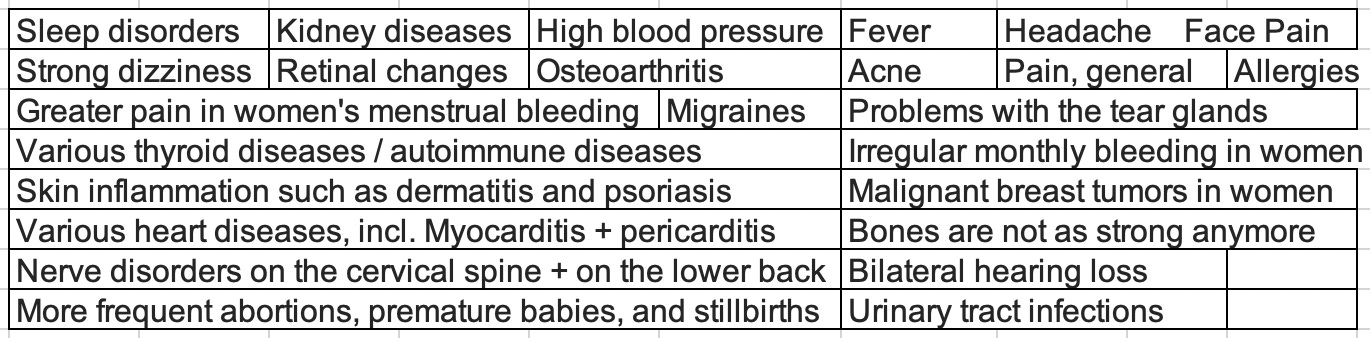
This concerning safety signal prompted one German Political Party, the AFD (a controversial right wing party that has gained appeal through opposing the mandates) to file the German equivalent of FOIA for the rest of the insurance data (note: a few longtime liberal friends in Germany who joined AFD believe “conservative” is a more appropriate label). Recently AFD obtained AOK Sachsen-Anhalt’s data, which once analyzed, demonstrated that many of the conditions we associate with COVID-19 injuries noticeably increased when the vaccination campaign initiated. According to this interview and Google translate, the conditions which rose five-fold or more were:
Today, the AFD hosted a press conference to unveil the data on 72 million patients (the 90% of Germans with statutory health insurance) they had obtained from KBV, the association which represents all physicians who receive insurance in Germany. This data summarizes the number of times all ICD-10 (an international standard) diagnostic codes were used by German healthcare providers for these patients (outside of hospitals) from the first quarter of 2016 to the first quarter of 2022.
Tom Lausen is a data activist who had previously revealed the PEI and the RKI (the German equivalent of the CDC) were concealing concerning vaccine safety data and was allowed to analyze both BKK and AOK’s data. For this presentation, Lausen was able to provide a preliminary summary of the KBV data a few days after it was released:
A rough translation of this presentation can be found here (additionally YouTube now will translate the subtitles). If this video is deleted it can also be found here.
A few of the points emphasized in this presentation include:
•The PEI and RKI had failed in their duty by federal law to evaluate COVID-19 vaccine injuries. Many of my friends and readers likewise believe they have done an atrocious job by attempting to conceal the vaccine injuries, and these agencies are frequently chastised by the German people for their conduct.
•It is estimated that 90% of the suspicious deaths that occur after vaccination are not reported to the PEI, and approximately 90% of those reported come from the patient themselves or their relative (which again demonstrates that German healthcare providers are failing in their duty to report vaccine injuries).
•The PEI has nonetheless received over 3,000 reports of suspicious deaths following vaccination, but lacks the authority to order autopsies and thus, has not performed them (fortunately as noted above, other groups have taken the initiative to do so).
For this press conference, a presentation was put together detailing Lausen’s preliminary findings and the correspondences with the regulatory agencies, all of which can be found here. To the best of my ability, I translated and slightly modified the key portions of the presentation so that they could be accessible to English speakers, but I am certain more will be translated in the upcoming days.
The KBV Data
All of the KBV data can be reviewed with a simple search tool here, although it does not seem to work for certain ICD-10 codes. Due to the importance of this data, for data preservation purposes, I am also providing a copy of the raw data the AFD received:
 Germany Total Icd 10 Code Submissions 2016 2022
Germany Total Icd 10 Code Submissions 2016 2022
1.87MB ∙ PDF File Download
This PDF file was supplied in a manner which appeared to be designed to make the data as difficult as possible to analyze. Fortunately, one of my readers was able to move the above file into an easily sortable spreadsheet and thereby address some of the challenges with the PDF:
German Data Sortable Sheet
3.06MB ∙ XLSX File Download
Finally, the above sheet was sorted by that reader into a smart spreadsheet which allows you to easily observe which codes had the greatest increase in 2021-2022 (e.g. to sort them or create graphs). For those of you who are data inclined, you will likely want to create this sheet yourself, but for everyone else this is an excellent reference to start with). They were also able to use a script to put about one third of the names for the ICD-10 codes, but since there are fifteen thousand of them, it wasn’t practical for us to manually add in the rest and you will frequently need to directly look up the codes themselves.
When building this, we came to the assessment that for each period in time (e.g., 2016 quarter 1), the German team added two different values together (code_20161 and nocode_20161). We are not sure what these two categories represent (an attempt to explain this is provided here) but we know the “nocodes” were necessary to reach the approximate levels of the conditions observed in the country at each point in time. Additionally, some of the extreme outliers exist because new ICD-10 codes are added each year and thus did not exist prior to 2021/2022. Finally, some of the codes you would expect to have large changes may not show in here if they are codes typically used in a hospital setting as this dataset does not include hospital coding.
Kbv Data Sorted Into Accessible Excel Sheet
9.46MB ∙ XLSX File Download
In the coming days, I know many will use this data to verify our work identifying which codes in 2021-2022 had the greatest increase (you can also do that piece by piece with the already available tool), and then cross reference those to the increases reported in VAERS or other datasets. There is an immense amount to be ascertained here, and I believe it represents the credible evidence we have been looking for since the start of the pandemic to have an objective metric for quantifying the impact of vaccine injury. However, it is also critical we assess that some of the observed trends are not due to artifacts within the data.

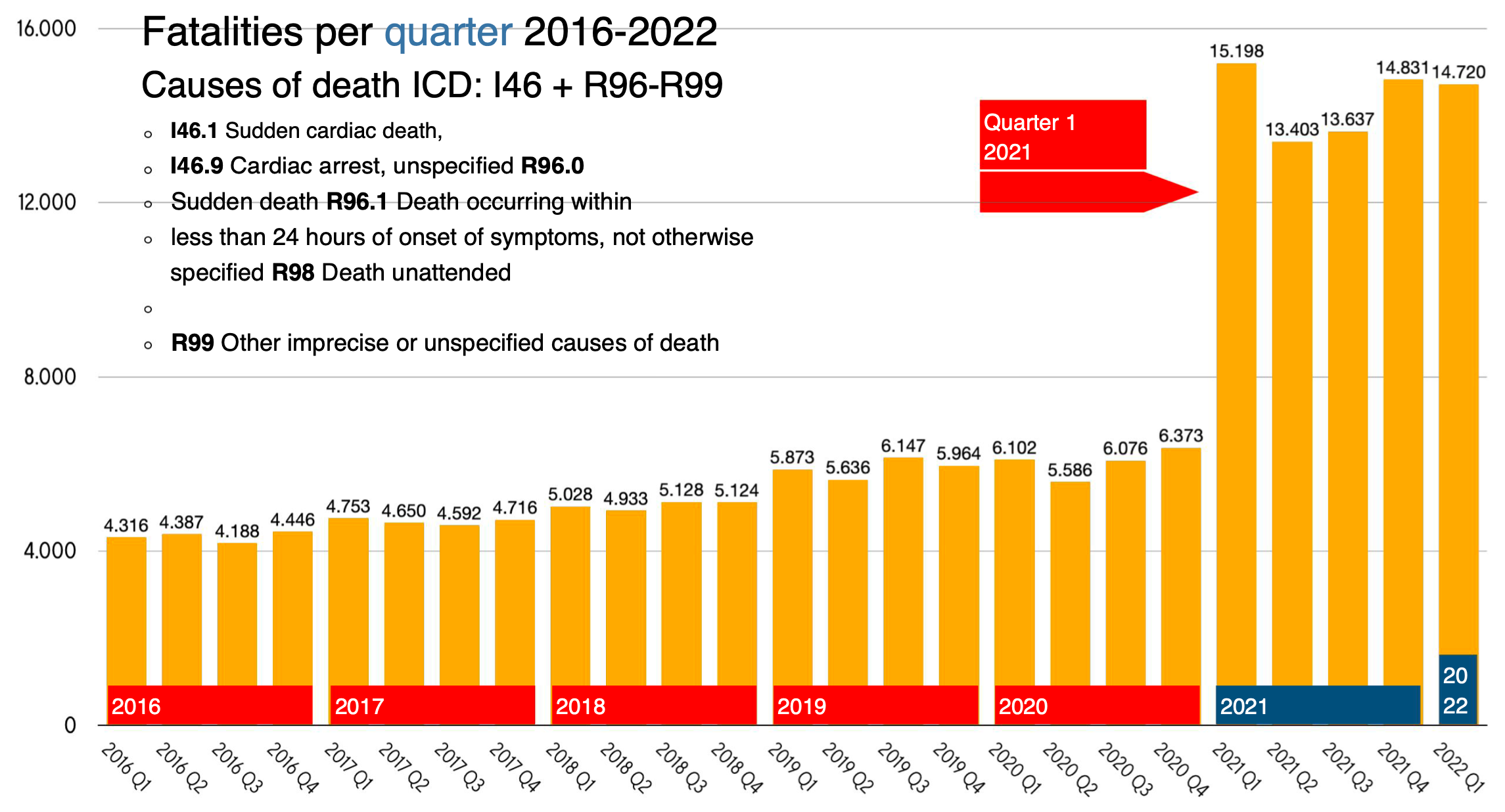
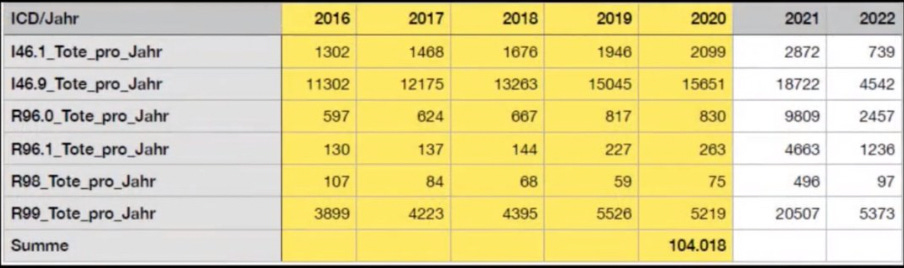
This is probably the most important graph of their presentation. We have all heard stories of individuals dying suddenly after vaccination (I’ve even read a report of an individual who appeared to be in good health making a thump in another room and being found dead shortly after by their spouse).
This issue was recently brought to the public’s attention with Died Suddenly, a documentary that effectively brought attention to this issue, but also had factual errors which were counterproductive for persuading the public that this issue is real. However, while some of the proof that Died Suddenly provided to assert the existence of the sudden death phenomenon could not stand up to outside scrutiny, the same cannot be said of the KBV data.
Additionally, one way that individuals have analyzed the unusual changes in health following the vaccination campaigns has been to assess how far they fall outside of the expected range of variation (this was also done for the final spreadsheet). I did a quick calculation for the above graph and found that 2021’s increase from 2016-2020 was 37.7σ, while 2022’s was 41.0σ. This is quite a big deal (the rarity of an event happening by chance increases exponentially as the σ increases). For context, a 7σ event has a 1/390,632,286,180 chance of spontaneously occurring (it is thought to occur once in a billion years), a 10σ event happens spontaneously once every 5.249e+020 years, and a 25σ event happens by chance every 1.309e+135 years (I was not able to find a reference on the probabilities for the even higher σ events observed here).
Given these numbers, it is very difficult to argue that these events were not caused by something. In this regard, we are also quite fortunate that while the vaccines were rushed to the market over a period of time far too short to establish safety, that process still took a year. Because of this lag, it is possible to refute the commonly cited argument that these changes were due to COVID-19 or the lockdowns, as these only occurred in 2020 (the only possible exception I can think of is that Delta emerged near the end of 2020, but the spike started well before Delta became prevalent in Europe later in 2021).
This is a similar graph to the previous one, but include sudden cardiac death, which as many of you know also “unexpectedly” increased.
For context, this was the rate of COVID vaccination in Germany:
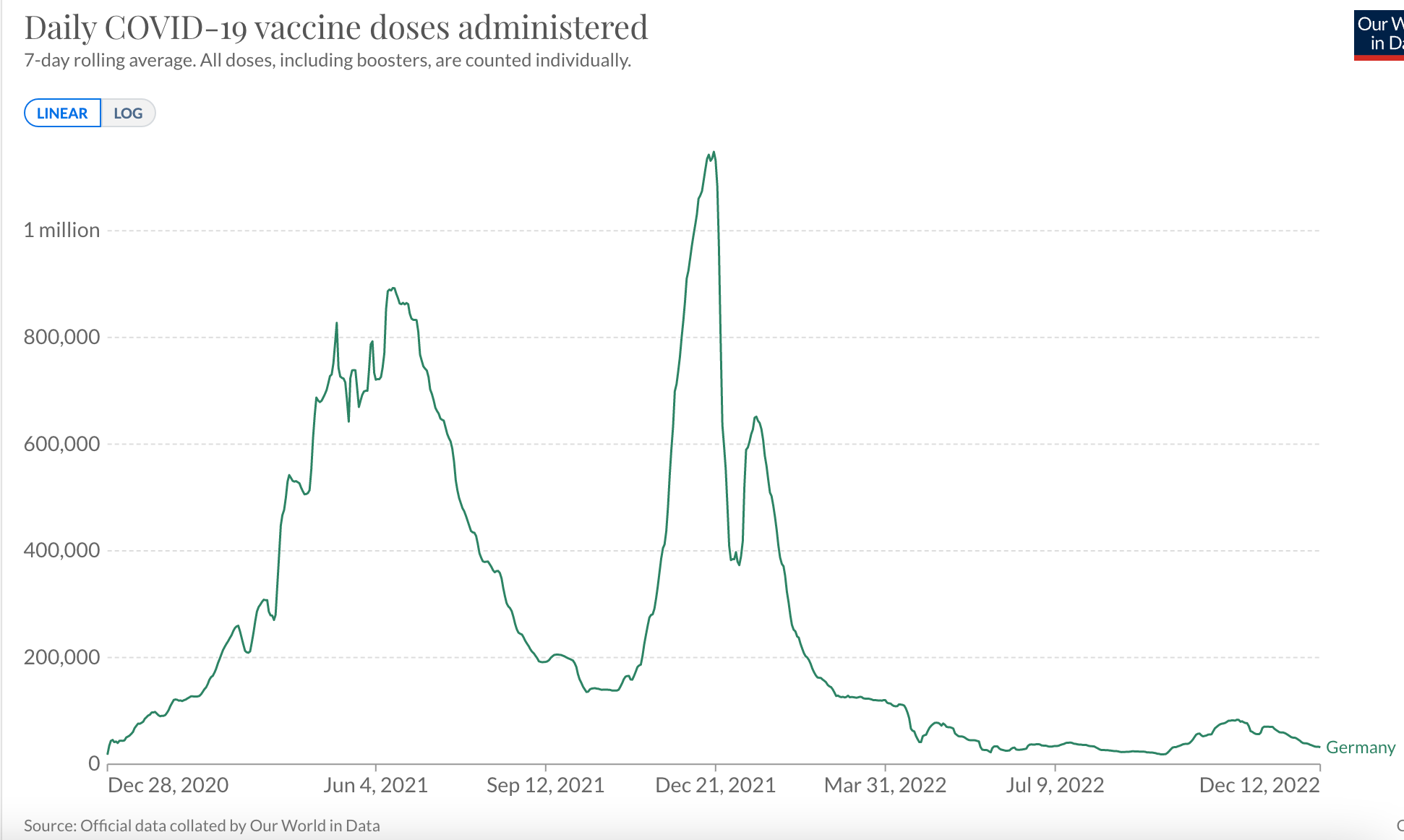
COVID-19 is not the only vaccination regularly received. For example in Germany in 2019, it was estimated that 39% of those 65 and older received an influenza vaccination. However, unlike previous vaccines, the introduction of the COVID-19 vaccine caused far more people to require medical care for a vaccine side effect.
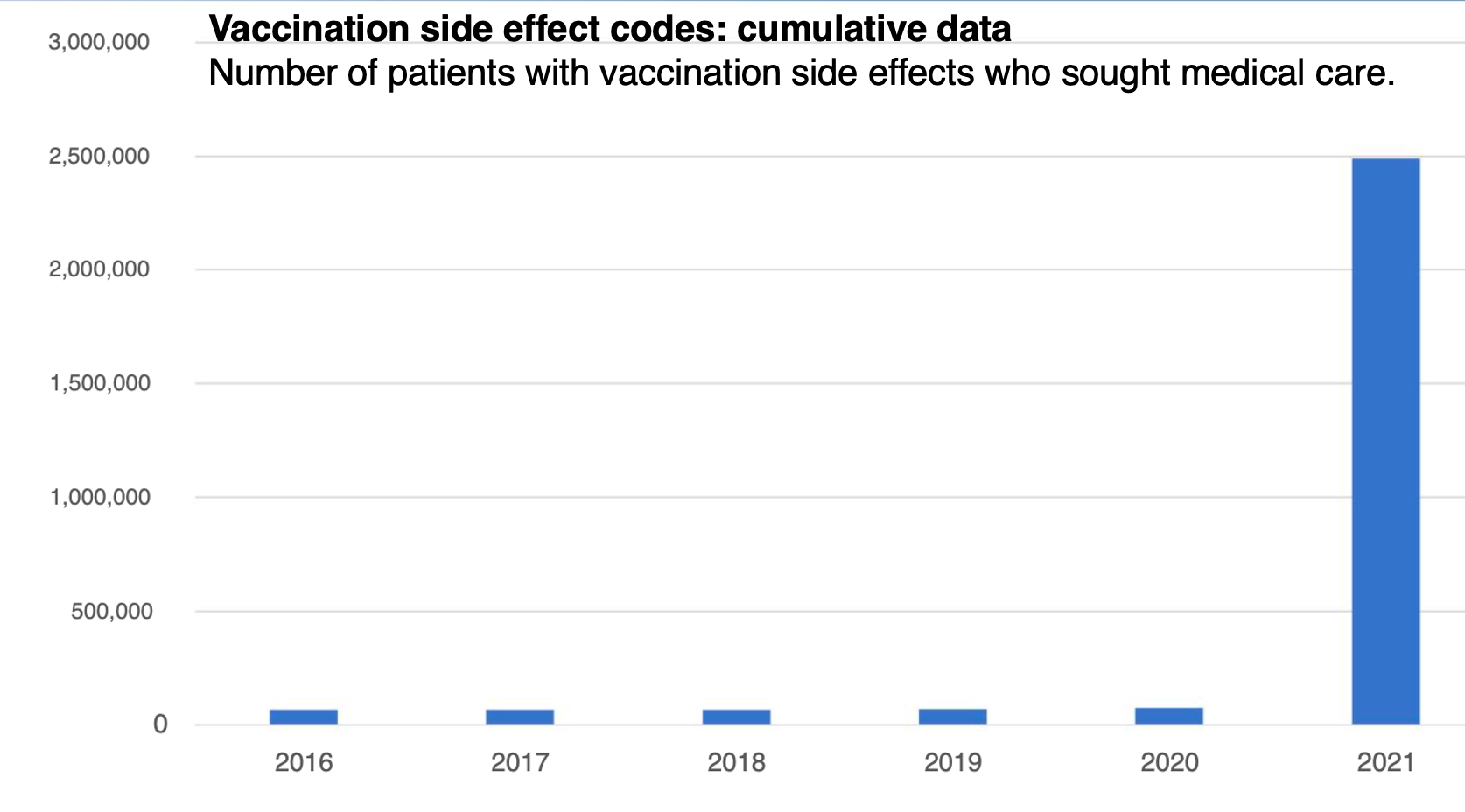
Given that Germany has a longstanding practice of tracking vaccine injuries, this graph makes a very important point. An actual increase in vaccine injuries is occurring and it is not a result of a bias leading to over-reporting; it is a result of the vaccines being dangerous and patients needing medical care for the injuries.
Given that there are thousands of ICD codes that I could search the database for (many other increases, such as those of certain cancers, were highlighted in Lausen’s presentation), I had to put some thought into which of those many increases would be the best to show for this article (there were a lot of compelling candidates).
Previously, I proposed a model for the unusual fibrous clots observed in Died Suddenly that revolved around spike proteins causing protein misfolding. In support of this model, I highlighted an observed increase of an extremely rare protein misfolding disease which continues to be reported in VAERS.
Creutzfeldt-Jakob disease typically develop over years and occurs in approximately one in a million people annually, making its occurrence immediately after vaccination rare to the point that suggests causation. The increase I proposed was a key point of contention for those who did not agree with my misfolded clot hypothesis, so I was eager to see if a current dataset could evaluate what was occurring.
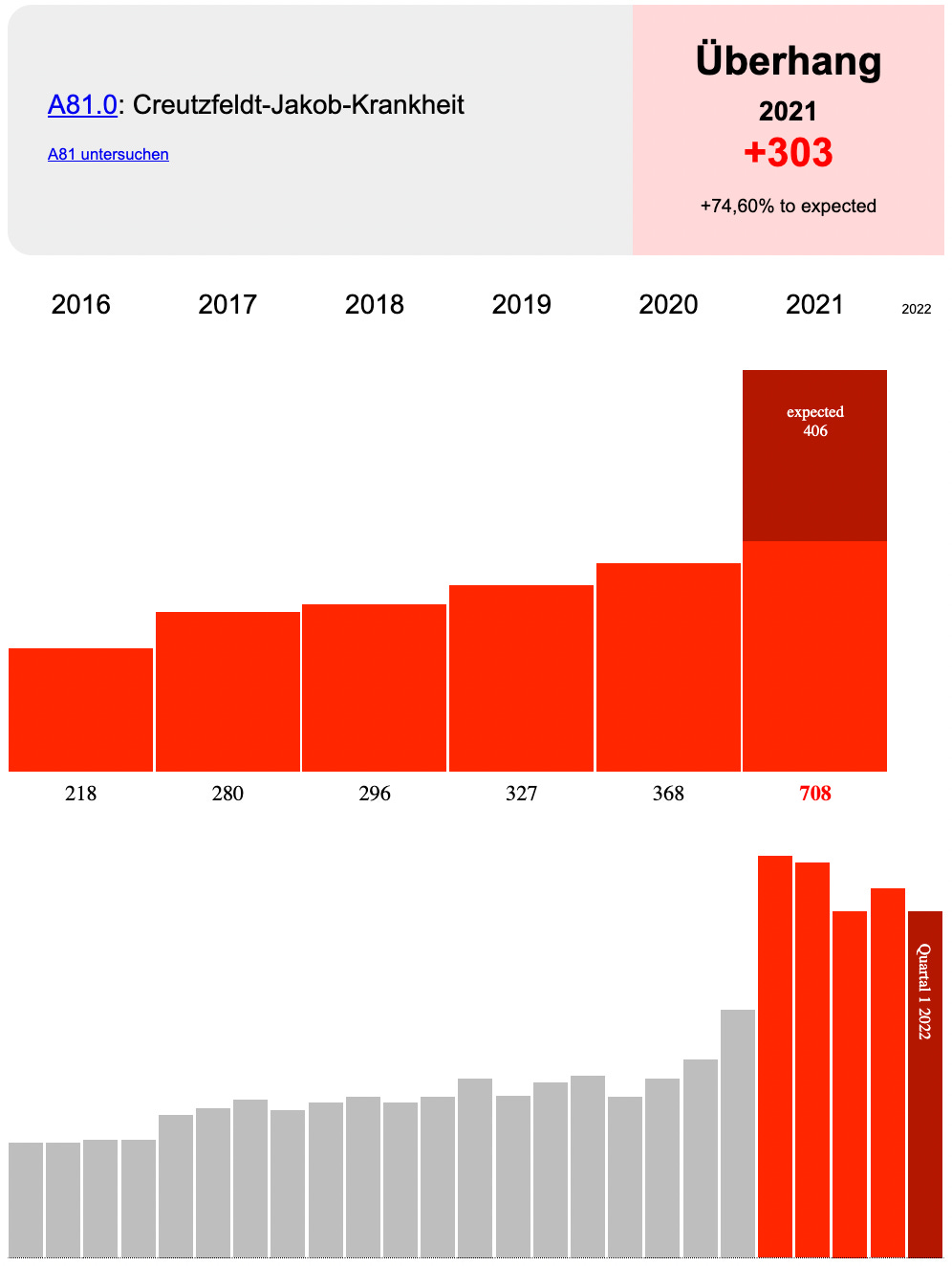
This increase is also quite large, and for all practical purposes impossible to have occurred by chance (although I will mention the authors who published the original case series linking COVID vaccination to 26 cases of CJD also determined that Delta appeared to have an increased capacity to trigger protein misfolding but I do not believe that can explain the above trend).
Finally, the presentation on the KBV data proposes a fatality rate for the COVID vaccines. I was not able to verify the methodology for this chart, but I inferred that it was derived from the death rates observed within the insurance data.
Is This Data Valid?
Following the AFD’s press conference, the leading medical research institute in Germany, ZI, acted as a third party to present a rebuttal of how AFD interpreted KBV’s data. I did not agree with their argument (that there results were an artifact of AFD also requesting for everyone who specifically died in 2021), but did note that their response acknowledged the authenticity of this data. The basis for my skepticism of this rebuttal was:
•German authorities having a long track record of attempting to cover up evidence of vaccine harm.
•Sudden deaths occurring on a consistent basis prior to 2021 in the dataset (this invalidates the argument ZI put forward which it “addressed” by saying those earlier deaths were due to data transmission errors).
•The large σ found for many, but by no means all non-fatal conditions in the dataset suggests that something besides artifacts relating to time of death is causing this discrepancy. However, it is also very possible some of the discrepancies present are due to not yet identified artifacts within the data.
A more detailed rebuttal of ZI’s arguments was posted here.
AFD also discussed the above rebuttal in a thread here stating:
“Hello all. The death-numbers that we have published are being hotly debated right now. Now the Central Institute for the KBV has joined in has said that the data we presented were quite easy to explain: ‘The data is only for people who have accessed a medical service in 2021 and only such people had been billed and therefore would be in the data and everything in the years before are statistical runaways. There are also different causes of death that were significantly higher in the years before such as I46.9 (heart attack without successful reanimation). ‘ All together 104 000 people have been coded as deaths in the years 2016-2020 of whom the Central Institute of the KBV now says that they were billed medical services in 2021. Now we have a question: If this is really true, we demand an explanation from the Central Institute of the KBV how 104 000 persons that have died in the years 2016-2020 have been billed medical services in 2021.” [Translated courtesy of a reader]
The following was also written in the tweet: “Allegedly, the figures from the KBV are only for patients with health insurance, for whom services were billed in 2021. However, the causes of death were coded for 104,000 patients in previous years. Do we have a data scandal or a billing scandal?”
Many of the German commentators I saw online were also skeptical of the official rebuttals to this data. I was recently sent a detailed summary of the events after the press conference I was sent recently demonstrated that the rationale for debunking it changed as time went forward. As best as I can tell, no clear reason was presented for why Lausen’s analysis was flawed given. Instead it was insinuated either that Lausen incorrectly filtered the data (we and others however arrived at the same results Lausen did) or that there was a data transmission error from the KBV (which is possible but would have had to have been deliberate or inconceivable incompetence).
KBV also issued an astonishing statement refuting AFD’s presentation:
The KBV board clarifies: Based on the billing data transmitted by the KBV to the AfD or. ICD-10 codes cannot be used to establish causal relationships between COVID-19 vaccinations and deaths. From the KBV’s point of view, the increase in deaths shown in quarters I-IV 2021 and quarter I 2022 is largely pandemic-related mortality. This once again illustrates the importance of COVID 19 vaccination as an effective measure to prevent serious forms of progress up to deaths. Without the vaccination, mortality would probably have been much higher.
This statement also cited the previously referenced ZI letter and another one which noted:
•The codes in this database do not include codes entered on death certificates and thus cannot be assigned as the cause of death [however all of these codes cannot be entered unless the patient died; also as the statement above shows KBV is admitting an increase in deaths occurred].
•The codes in this database cannot be correlated with vaccination status because many people received the COVID vaccines in settings that did not result in codes being submitted and coding for COVID vaccination has not yet been included in the dataset due to special regulations [I agree, but we can still observe changes within the entire population].
•This database was not created for the purpose of conducting medical research and therefore no conclusion can be drawn from it [I don’t believe this is a valid argument].
From my perspective, none of the above points refute the sudden increases in submitted billing codes (hypothesized to correlate with vaccine injuries) that occurred a year after the pandemic started at the exact same time the vaccination campaign began. However, I also believe some type of not yet identified artifact could account for at least some of what was observed. If anyone can provider a stronger refutation of the data presented here (preferably, at the pinned comment), I would greatly appreciate it. We need to help each other stay honest and I will gladly retract this article if a critical mistake was made.
Conclusion
Given the extremely concerning implications of the German data, it is not surprising that governments around the world and healthcare systems or insurance providers have been reluctant to release their own data. It is my sincere hope that this release will open the flood gates to additional disclosures and I am in complete agreement with the conclusion of this presentation:

I wish we had an American political party stating the same. There are signs of hope however; today Ron DeSantis did something incredible and requested a grand jury against Pfizer and Moderna, an essential step a few leaders in our movement have been working to lay the groundwork for over the last two years. I am also hopeful that this grand jury will compel the state of Florida to release similar data that can be used to assess the safety of these vaccines.
I strongly encourage those of you who who are able to begin looking through the KBV dataset and identifying important trends that can be correlated to other observations we have made over the last two years. I believe there are many excellent articles that could be written on them. I sincerely thank all of you for your continued support!
My primary goal is to draw attention to this data so numerous independent parties can objectively analyze it and independently verify if the trends it shows correlate to “controversial” increases observed in other datasets like VAERS. This data is extremely important as it is the only access we have ever been given to observe the changes in illness that follow the COVID vaccination campaigns. I also suspect the most important use of this data will be to establish causality for specific vaccine injuries.
This matters because typically when someone suffers a pharmaceutical injury, it is not acknowledged by the the government and the courts because “there is no evidence the product is associated with that injury,” and as you might expect, the pharmaceutical industry work tirelessly to make sure the evidence that could implicate their product never emerges.
At this point I’ve lost track of how many sad instances I’ve seen where this happened to a medically injured patient (in some cases to the point the gaslighted victim gives up and ends their lives), so I greatly support having an independent means to assess casualty for vaccine injuries. Those injured by the COVID-19 vaccines are profoundly suffering and they really need help (on the bright side however, recently Senator Johnson and shortly after Governor DeSantis gave a voice to these victims).
Thank you as always for your support and I will continue working to update this article as more information becomes available.
Postscript: It appears a similar rise in unexplained deaths is occurring in Canada.
https://amidwesterndoctor.substack.com/p/the-most-important-dataset-of-the
_______________________________
The Time for Silence is Over
A unified pushback against the globalist agenda
It’s finally here, the Global Walkout begins September 4th at 8pm London time and continue every weeks. Next step january 8th.
One step at a time, hand in hand, we are walking out from the globalist society they are trying to enslave us into
ANYONE can participate
ANYWHERE in the world
JOIN or read about it here – https://globalwalkout.com

https://www.reignitefreedom.com/
The third step is to unsubscribe from all mainstream media outlets. Delete the apps from your phone, laptop, and tablet and unfollow all of their social media and YouTube channels. Try to avoid mainstream media for at least one week, even if the headline is intriguing.
In the same time why not removing all the big tech tracking/spying/social credit system around you: (Youtube, Facebook, Instagram, Twitter, Tik Tok, Google, Apple, Microsoft, Whatsapp, Zoom, Linkedln, Snapchat, Tumblr, Pinterest, Reddit, Myspace, etc.)
The fourth step of the global walkout is to move as many accounts as you can to a union or local bank.
If you like our work please consider to donate :
_______________________________
If you are looking for solutions (lawyer, form, gathering, action, antidote, treatments, maybe this could help you:
HERE
If you want to fight back better:
https://childrenshealthdefense.org/child-health-topics/health-freedom/defender-days-sticker-gallery/
Find the others: www.freedomcells.org
Spike Protein Protocol
Glutathione (most important for body detoxification) or better
NAC = N-Acetyl-Cysteine 600-750mg (causes the body to produce glutathione itself)
Zinc
Astaxantin 5mg (also improves vision)
Quercetin
vitamin D3
Milk thistle (also liver and stomach protection)
Melatonin 1mg to 10mg (against 5G)
Alternatively CDS/CDL and zeolite
Dr. Zelenko’s Protocol contains Ivermectin, Hydroxychloroquine (HCQ), Zinc, Vitamin D3, and Quercetin.
How to find the truth :
Search engine: https://metager.org/ https://presearch.org/ or https://search.brave.com/
Videos: www.brandnewtube.com
www.odysee.com
www.bitchute.com
Facebook style: www.gab.com
INTELLIGENCE ISN’T KNOWING EVERYTHING, IT’S THE ABILITY TO CHALLENGE EVERYTHING YOU KNOW
 Posted in
Posted in  Tags:
Tags: 













