 RSS Feed
RSS Feed















 January 24th, 2024
January 24th, 2024  Awake Goy
Awake Goy During 2020-2023, professional regulatory associations became de-facto wardens of the more authoritarian Covid-19 nation-states, which included New Zealand. The Medical Council of New Zealand (MCNZ) was one such body which, like a duck to water, moved firmly and swiftly to ensure that doctors complied with Covid-19 and vaccine policies, or face disciplinary proceedings and gag orders.
In an era when institutional trust is declining, the MCNZ didn’t apparently recognise the cognitive dissonance created by two contradictory 2021 guidance papers. They certainly didn’t consider that their ideological suppression of medical doctors when it came to Covid-19 matters might imply that doctors might not be trusted on other matters, either. The Medical Council also appeared blithe to the impact of ‘lost’ doctors in an already stressed and under-resourced medical system.
The Ministry of Health provided the carrot, incentivising compliance by funding doctors to both diagnose SARS-CoV-2 infection and to inject Pfizer’s BNT162b2 gene therapy into their arms, and the MCNZ provided the stick, by roundup.
Covid-19 was the exception. The MCNZ’s April 2021 guidance statement (revoked in September 2023) stated that there was:
no place for anti-vaccination messages in professional health practice, nor any promotion of anti- vaccination claims including on social media and advertising by health practitioners.
From 2021 onwards, dozens of doctors were investigated, put in front of an MZNZ tribunal and many doctors had their medical licenses suspended.
MCNZ’s June 2021 guidance statement (the ‘rule’) – set ‘out the standards of good medical practice when discussing options for treatment and obtaining consent from patients.’ The process of obtaining the permission, called informed consent, was in place to:
help the patient decide whether they want a treatment, they first need to be given information, such as the risks and benefits of their treatment options.
As the MCNZ stated, a key principle of informed consent ‘is trust.’
Trust is essential in the doctor-patient relationship. One way to build trust is to provide information openly and honestly to your patient.
For properly informed consent, doctors ‘must give your patient the information they need to help them make a fully-informed decision;’ and ‘[s]hare information that is relevant to them, in a way they understand, and allow reasonable time for the patient to make their decision.’
Without a hint of irony, doctors were urged to question ‘whether there is anything else you can do to make it easier for your patient to consider the different options and make a fully informed decision.’ They were advised to ‘[b]e open and honest with your patient, and answer their questions accurately’ and take ‘into account your patient’s cultural, religious, and social needs, and their values and beliefs.’ Doctors should consider whether they had ‘explained the different treatment options including the risks and benefits of each option, and the option of not treating (adopting a see what happens with time approach)?’
Of course, doctors had ‘a special duty of care when enrolling patients into immunisation or screening programmes. This includes making the person aware of any limitations of a screening programme and the uncertainties, in particular the chance of false positive and false negative results.’
The informed consent information process was designed to foster trust between doctor and patient and encouraged free and frank information flows to nurture that trust. MCNZ’s actions in rounding up and disciplining doctors over that same period, from mid-June 2021- January 2022, spectacularly collided with their own guidance instructions for informed consent.
The informed consent process guidance paper was released as Covid-19 mandate crackdowns tumbled out through Cabinet’s secretive, delegated legislation process.
Contradictorily and hypocritically, openness and honesty were quashed where Pfizer’s BNT162b2 gene therapy was concerned. Pfizer’s new technology was ‘command medicine.’ Uncomfortable, uncertain and contradictory discussion was interdit.
New Zealand doctors whose behaviour was inconsistent with the New Zealand government’s Covid-19 policy and found to be ‘guilty’ by the MCNZ were required to sign a ‘voluntary undertaking and undertake an ‘Educational Programme.’
The programme included ‘educational activities’ and compulsory supervision. The ‘supervisor’ was required to undertake pharmacological reviews and oversee the doctors prescribing practices. They were given the powers, much to the horror of many doctors, to randomly check the ‘quality of the notes.’ Cite confidential patient records. The supervisor would then report back to the MCNZ on a monthly basis.
The ‘Voluntary Undertaking’ that recalcitrant doctors were required to sign carried with it all the power of a gag order. The ‘undertaking’ prevented doctors from providing ‘their view, or the views of others with similar views’ about vaccination or immunisation against Covid-19.
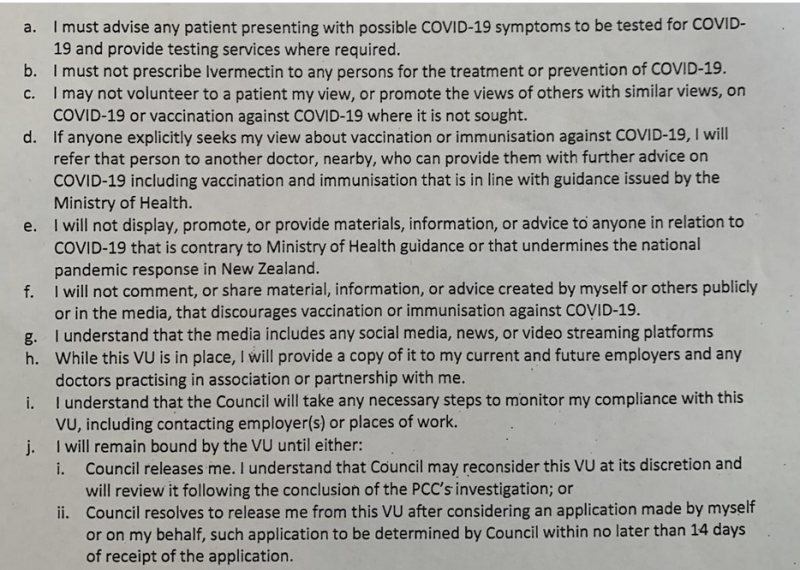

Nothing could be spoken or published that was:
contrary to Ministry of Health guidance or that undermines the national pandemic response.
The MCNZ were instructing doctors to deliberately suppress scientific information. We can presume that the ‘views of others’ includes that of expert scientists who publish in the scientific literature.
And no matter the evidence or safety profile of Ivermectin, it must not be prescribed for Covid-19.
The actions of the MCNZ effectively inserted the New Zealand government inside the doctors’ practice room, between the patient and the doctor.
This was enabled, most powerfully, by threatening the suspension of the medical licenses of dissenting doctors. The MCNZ exploited their powers to take the ability to practice medicine away from New Zealand doctors.
Doctors had to acquiesce to the ‘Educational Programme’ if they were to retain their ability to practice medicine:


Doctors were required to pay for the costs of the supervisor, another medical doctor. The ‘Educational Programme’ was presumed to fit around the administrative burden of their medical clinics and the extraordinary patient demands in a pandemic emergency.
If the demands of the MCNZ were to be satisfied.
This included a requirement that doctors review prescribed reading material once a month, taking notes as proof the papers had been read. Most of the literature was published during Covid-19:
Reifying a static concept of ‘consensus’ that presents all scientists who disagree with ‘consensus’ as outsiders appears quite popular. These behavioural and psychological scientists seem reluctant to wrangle with eminently sociological issues. This includes Mertonian concepts such as ‘organised skepticism’ and the incentivised reward systems that inevitably impose norms and values upon the scientists who inhabit them. From which ‘peers’ are included, to the terms of reference for what ‘evidence’ would be considered legitimate, and the resourcing for research and review. What is excluded as ‘specified ignorance’ affects the trajectory of knowledge, just as much as what is included.
For anyone who has read Orwell and Huxley, the Educational Programme papers; the inferential basis of what ‘scientific facts’ were; and the ‘voluntary’ coercion imposed on doctors – was all mind-bogglingly eye-popping.
Power is in tearing human minds to pieces and putting them together again in new shapes of your own choosing.
George Orwell, 1984
The MCNZ’s enforcement actions appear, from the time they were imposed in 2021, until 2023 when they quietly withdrew the ‘Guidance,’ demeaning, unethical, totalitarian, and short-sighted.
I say totalitarian, because the bulk of information the government relied on came either directly from Pfizer, or from other regulatory agencies who also relied on information directly from Pfizer. These arrangements were never transparent or accountable. They were never democratic.
Doctors were caught up in the maelstrom. If doctors rejected the commands, they would lose their medical licenses. In a country where securing doctors with a long history of service with expertise in remote and low-income regions was difficult – these doctors knew that in many ways, their patients would suffer. It was not only the prescribing history. Long-term relationships take time to develop, but these are the basis of trust-based decision-making. They are the heart of medical practice.
It’s necessary to turn our minds back and revisit the fear campaign around SARS-CoV-2 infection that drenched legacy media over this period. New Zealand media absented itself from even-handedly discussing information that contradicted central governments’ political position.
The MCNZ is not a scientific organisation. Their position on risk was informed by the New Zealand governments’ position on risk.
The campaign against dissenting doctors was deliberate and political. The period from when complaints against doctors and suspensions of medical licenses peaked occurred when a significant body of growing scientific information contradicted the persistent claim, by the Prime Minister, the Minister for Covid-19 and the Ministry of Health, that Pfizer’s BNT162b2 gene therapy was safe and effective.
The predetermined vaccine rollout programme, established prior to March 2021, could not be disrupted.
Doctors who contradicted the New Zealand government’s political position were accused of ‘peddling misinformation.’ The New Zealand media dutifully amplified the MCNZ’s zero tolerance message and called cautious doctors ‘anti-vax GPs.’ Media vilification extended to doctors who advised that pregnant women and young people approach Covid-19 vaccination cautiously.
Notwithstanding that by April 2020, a large body of information, held by both military and public health scientists, had largely confirmed that the elderly and infirm and those with multiple debilitating health comorbidities were most at risk.
But the New Zealand public did not know this. Nor did, evidently, the New Zealand government. New Zealand’s Covid-19 information strategies excluded and short-circuited good process. There was no independent public research institution with either the capacity or the obligation to routinely and methodologically evaluate the ever-changing evidence.
Neither the TAG’s, the expert advisory groups; nor the so-called risk modellers who dominated the ‘evidential reasoning’ space, were doing this research. No one looked at age-stratified risk. Sero-prevalence studies were never publicly disclosed, and the Coroner had no processes to determine whether a death was caused by Covid-19 or by the medical intervention.
An epidemiologist who had spent time analysing the scientific literature to analyse how scientists and researchers – globally – were depicting safety and efficacy of this novel genetic technology was warned by lawyers not to speak publicly.
The broad public and institutional ignorance effectively, as Wynne put it, ‘exogenised’ the uncertainties. The vaccine was only ever safe and effective. Indeed, plausibility, not science dominated public discussions on Covid-19.
When doctors stepped in to address the informational gap, they were pilloried for it. These doctors were, almost daily, reviewing literature and discussing global findings with their colleagues. I got to speak with them and confirm this at the NZDSOS conference, held last year in Auckland.
None of the doctors in the naughty corner had ever been reported prior to the MCNZ landing on them, like the veritable tonne of bricks. All had busy clinical practices up until their suspension, and had practiced for between 20 and 40 years. Their records were exemplary.
Ethically, if New Zealand doctors were to appropriately follow the informed consent guidelines, they should have had the autonomy to judge the already known risk profile of BNT162b2, and balance it against a patient’s risk profile.
However, this was not permitted by the legally and administratively focussed MCNZ.
These doctors were not vulnerable early or mid-career medics with large debts. Because they were no longer mid-career with young families, many of these doctors spent evenings trawling the scientific literature and speaking with colleagues locally and globally.
Perhaps they saw the silences in government and media in 2020 when Imperial College London overpredicted death rates, while high-calibre epidemiologists took a milder view. Perhaps their doubt was seeded by entrenched financial conflicts of interest, from the influential billionaires, to the politicians and regulators in the US and the United Kingdom.
These doctors understood the triple jeopardy faced by their immunosuppressed patients. They were most at risk of serious Covid-19 and most at risk of any vaccine not working and at risk of harm from an adverse event.
These doctors were painfully aware that many of their patients were already on complex drug regimes. They did not need another drug-related (iatrogenic) adverse event. This explains why many wanted to use nutrients and medicines with a long history of use and an excellent safety profile such as the blackballed ivermectin. Why they considered it critical to provide nutrients (such as zinc and vitamin D) that would buffer immune systems, and antivirals to prevent illness cascades (and assist immune-protective zinc to enter cells, which is what ivermectin does).
Perhaps these doctors understood that precaution was warranted because biologic drugs are unstable and at extraordinary risk for variability due to the presence of organic/biological material. It has only been revealed in 2023 that the batches rolled out globally were made using different processes and that other (not-declared) DNA fragments were present in the vaccine vials.
Whatever was known in 2021, these doctors definitely understood the vast uncertainty accompanying the prescribing of a brand-new drug that hadn’t undertaken long-term safety trials. That greater drug risk lay with healthy young people and pregnant women – for if the drug was harmful (unlike someone in end-of-life care), the suffering could roll on for decades.
For these doctors, these issues were part of the relevant considerations they took into account, as their patients walked through their clinic door. And quietly, for these doctors, these issues were personal, for them too.
For this work they were at risk of being reported by colleagues, by patients, and by patients’ families. These doctors had decades of experience at the front lines in flu season. They had spent their life delicately managing the biopsychosocial world that is, and always was, contained in every patient to present in their clinic.
We can only wonder what relevant considerations were taken into account by the MCNZ, a member organisation of the US-based Federation of State Medical Boards (FSMB), when it developed and published its Guidelines – which for New Zealand doctors, carried all the force of law. But of course, because they’re a private organisation, we can’t make an Official Information Act request to find out.
In July 2021 the FSMB released a statement stating:
Physicians who generate and spread Covid-19 vaccine misinformation or disinformation are risking disciplinary action by state medical boards, including the suspension or revocation of their medical license.
We can only wonder to what extent replica instructions rolled out globally. Did other FSMB member organisations require doctors to comply with the rigors of a so-called ‘Educational Programme?’
New Zealand was always vulnerable to an informational coup. A constellation of countervailing powers arguably prevented doctors from meaningfully altering the Covid-19 ‘safe and effective’ hard line position. We can see, in the Cabinet minutes in 2020, before the vaccine was released, the political and cultural ushering in of the whole of government to a language that would eternally, come hell or high water, place the text ‘safe and effective’ before the text ‘vaccine.’
For 30 years investigative journalism in the legacy media has died a painful death, while publicly-paid media persistently decline to deviate from the long-standing policy positions of central government.
Stakeholders in New Zealand do not tend to include the general public.
The stakeholders in Covid-19 included Pfizer; the financially incentivised media; the single-party Cabinet; a unicameral Parliament that was whipped into acquiescence; the colluding Ministries; the Medical Council of New Zealand; and a small cadre of expert scientists. It was these scientists whom judges persistently deferred to in court cases, even when plaintiffs’ scientists had greater subject matter expertise.
The medical doctors of New Zealand were not considered stakeholders during the Covid-19 pandemic. Au contraire, it was the job of the MCNZ to keep them in line.


 Posted in
Posted in  Tags:
Tags: 













