 RSS Feed
RSS Feed

















 October 23rd, 2023
October 23rd, 2023  Awake Goy
Awake Goy 
#ExcessDeaths
(August 2023): The International Olympic Committee reports that between 1966 and 2004, an average of 29 pro athletes each year died suddenly, “predominantly caused by pre-existing congenital cardiac abnormalities.” But since the COVID vaccine roll-out, over 1,400 pro athletes have died in 2021, 2022, and 2023 alone, as of August 2023. This is an enormous over ten-fold jump in magnitude, per year, on average.
GoodSciencing.com reports:
“The International Olympic Committee in Lausanne, Switzerland, studied documents from international data banks from 1966 to 2004. Those documents indicate 1,101 sudden deaths in athletes under 35 years of age, over 38 years, an average of 29 athletes per year, the sports with the highest incidence being soccer and basketball. Note the document says those sudden deaths were “predominantly caused by pre-existing congenital cardiac abnormalities.…
“…96 were reported in the month of January 2022 alone, 416 in 2021, 791 in 2022 and 138 in 2023. None of these new deaths were reported to be due to congenital abnormalities, the primary cause found in previous years.”
In her rebuttal to British MP Andrew Bridgen’s recent speech on COVID vaccines and the last two years’ explosion of non-COVID, unexplained excess deaths in the UK and around the world, MP Maria Caulfield tried to bat away MP Bridgen’s searing indictment of the COVID vaccine roll-outs as the culprit by blaming the flu and other diseases
Caulfield said
“I will start with winter flu. The number of positive tests last year peaked at 31.8%, the highest figure seen in the last six years. Interim analysis from the UKHSA indicates that the number of deaths in England associated with flu was far higher than pre-pandemic levels, so the excess deaths due to flu last winter are, sadly, part of the answer.”
Read Next Article:
Transcript: MP Andrew Bridgen on Government and Media Silence on Sky-High Non-COVID, Vaccine-Related Deaths, in UK and World
UK Parliament Official Transcript:
October 20, 2023
We have experienced more excess deaths since July 2021 than in the whole of 2020. Unlike during the pandemic, however, those deaths are not disproportionately of the old. In other words, the excess deaths are striking down people in the prime of life, but no one seems to care. I fear that history will not judge this House kindly. Worse still, in a country supposedly committed to the free and frank exchange of views, it appears that no one cares that no one cares. Well, I care, Mr Deputy Speaker, and I credit those Members in attendance today, who also care. I thank the hon. Member for Lincoln (Karl MᶜCartney) for his support, and I am sorry that he could not attend the debate.
It has taken a lot of effort, and more than 20 rejections, to be allowed to raise this topic, but at last we are here to discuss the number of people dying. Nothing could be more serious. Numerous countries are currently gripped in a period of unexpected mortality, and no one wants to talk about it. It is quite normal for death numbers to fluctuate up and down by chance alone, but what we are seeing here is a pattern repeated across countries, and the rise has not let up.
I commend the hon. Member for the tenacious way in which he has battled on this issue; I admire him for that. I wonder where he found the media were in all this. During the covid pandemic, every day the media—particularly the BBC—could not wait to tell us how many people had died on that particular day, without any context for those figures whatsoever, but they seem to have gone strangely quiet over excess deaths now.
I thank the hon. Gentleman for his intervention. He is absolutely right: the media have let the British public down badly. There will be a full press pack going out to all media outlets following my speech, with all the evidence to back up all the claims I will make, but I do not doubt that there will be no mention of it in the mainstream media.
One might think that a debate about excess deaths would be full of numbers, but this speech does not contain many numbers, because most of the important numbers are being kept hidden. Other data has been oddly presented in a distorted way, and concerned people seeking to highlight important findings and ask questions have found themselves inexplicably under attack.
Before debating excess deaths, it is important to understand how excess deaths are determined. To understand whether there is an excess, by definition, we need to estimate how many deaths would have been expected. The Organisation for Economic Co-operation and Development uses 2015 to 2019 as a baseline, and the Government’s Office for Health Improvement and Disparities uses a 2015 to 2019 baseline, modelled to allow for ageing. I have used that data here. Unforgivably, the Office for National Statistics has included deaths in 2021 as part of its baseline calculation for expected deaths, as if there was anything normal about the
Toggle showing location ofColumn 561
deaths in 2021. By exaggerating the number of deaths expected, the number of excess deaths can be minimised. Why would the ONS want to do that?
There is just too much that we do not know, and it is not good enough. The ONS publishes promptly each week the number of deaths registered. While that is commendable, it is not the data point that really matters. There is a total failure to collect, never mind publish, data on deaths that are referred for investigation to the coroner. Why does that matter? A referral means that it can be many months—or, given the backlog, many years—before a death is formally registered. Needing to investigate the cause of a death is fair enough, but failing to record when the death happened is not.
Because of that problem, we have no idea how many people died in 2021, even now. The problem is greatest for the younger age groups, where a higher proportion of deaths are investigated. This data failure is unacceptable and must change. There is nothing in a coroner’s report that can bring anyone back from the dead, and those deaths should be reported. The youngest age groups are important not only because they should have their whole lives ahead of them. If there is a new cause of excess mortality across the board, it would not be noticed so much in the older cohorts, because the extra deaths would be drowned out among the expected deaths. However, in the youngest cohorts, that is not the case.
There were nearly two extra deaths a day in the second half of 2021 among 15 to 19-year-old males, but potentially even more if those referred to the coroner were fully included. In a judicial review of the decision to vaccinate yet younger children, the ONS refused in court to give anonymised details about those deaths. It admitted that the data it was withholding was statistically significant. It said:
“the ONS recognises that more work could be undertaken to examine the mortality rates of young people in 2021, and intends to do so once more reliable data are available.”
How many more extra deaths in 15 to 19-year-olds will it take to trigger such work? Surely the ONS should be desperately keen to investigate deaths in young men. Why else do we have an independent body charged with examining mortality data? Surely the ONS has a responsibility to collect data from coroners to produce timely information.
Let us move on to old people. Most deaths in the old are registered promptly, and we have a better feel for how many older people are dying. Deaths from dementia and Alzheimer’s show what we ought to expect: there was a period of high mortality coinciding with covid and lockdowns, but ever since, there have been fewer deaths than expected. After a period of high mortality, we expect and historically have seen a period of low mortality, because those who have sadly died cannot die again.
Those whose deaths were slightly premature because of covid and lockdowns died earlier than they otherwise would have. That principle should hold true for every cause of death and every age group, but that is not what we are seeing. Even for the over-85-year-olds, according to the Office for Health Improvement and Disparities, there were 8,000 excess deaths—4% above the expected levels—for the 12 months starting in July 2020. That
Toggle showing location of Column 562
includes all of the autumn 2020 wave of covid when we had tiering and the second lockdown and all of the first covid winter. However, for the year starting July 2022, there were more than 18,000 excess deaths in this age group—9% above expected levels. That is more than twice as many in a period when there should have been a deficit and when deaths from diseases previously associated with old age were fewer than expected. I have raised my concerns about NG163 and the use of midazolam and morphine, which may have caused—and may still be causing—premature deaths in the vulnerable, but that is, sadly, a debate for another day.
There were just over 14,000 excess deaths in the under 65-year-olds before vaccination from April 2020 to the end of March 2021. However, since that time, there have been more than 21,000 excess deaths, ignoring the registration delay problem, and the majority of those deaths—58% of them—were not attributed to covid. We turned society upside down before vaccination for fear of excess deaths from covid, but today we have substantially more excess deaths, and in younger people, and there is a complete eerie silence. The evidence is unequivocal. There was a clear stepwise increase in mortality following the vaccine roll-out. There was a reprieve in the winter of 2021-22 because there were fewer than expected respiratory deaths, but otherwise the excess has been incessantly at this high level.
Ambulance data for England provides another clue. Ambulance calls for life- threatening emergencies were running at a steady 2,000 calls a day until the vaccine roll-out. From then, they rose to 2,500 daily, and calls have stayed at that level since. The surveillance systems designed to spot a safety problem have all flashed red, but no one is looking. Claims for personal independence payments from people who have developed a disability and cannot work rocketed with the vaccine roll-out and have continued to rise ever since. The same was seen in the US, which also started with the vaccine roll-out, not with covid. A study to determine the vaccination status of a sample of such claimants would be relatively quick and inexpensive to perform, yet nobody seems interested in ascertaining this vital information. Officials have chosen to turn a blind eye to this disturbing, irrefutable and frightening data, much like Nelson did—and for far less honourable reasons. He would be ashamed of us.
Furthermore, data that has been used to sing the praises of the vaccine is deeply flawed. Only one covid-related death was prevented in each of the initial major trials that led to authorisation of the vaccines, and that is taking the data entirely at face value, whereas a growing number of inconsistencies and anomalies suggest that we ought not to do this. Extrapolating from that means that between 15,000 and 20,000 people had to be injected to prevent a single death from covid. To prevent a single covid hospitalisation, more than 1,500 people needed to be injected. The trial data showed that one in 800 injected people had a serious, adverse event, meaning that they were hospitalised or had a life-threatening or life-changing condition. The risk of this was twice as high as the chance of preventing a covid hospitalisation. We are harming one in 800 people to supposedly save one in 20,000. That is madness.
The strongest claims have too often been based on modelling carried out on the basis of flawed assumptions. Where observational studies have been carried out,
Toggle showing location ofColumn 563
researchers will correct for age and comorbidities to make the vaccines look better. However, they never correct for socioeconomic or ethnic differences as that would make vaccines look worse. That matters. For example, claims of higher mortality in less vaccinated regions of the United States took no account of the fact that this was the case before the vaccines were rolled out. That is why studies that claim to show that the vaccines prevented covid deaths also showed a marked effect of them preventing non-covid deaths. The prevention of non-covid deaths was always a statistical illusion and claims of preventing covid deaths should not be assumed when that illusion has not been corrected for. When it is corrected for, the claims of efficacy for the vaccines vanish with it.
Covid disproportionately killed people from ethnic minorities and lower socioeconomic groups during the pandemic. In 2020, deaths among the most deprived were up by 23% compared with 17% for the least deprived. However, since 2022 the pattern has reversed, with 5% excess mortality among the most deprived compared with 7% among the least deprived. These deaths are being caused by something different.
In 2020, the excess was highest in the oldest cohorts, and there were fewer than expected deaths among younger age groups. However, since 2022, the 50 to 64-year-old cohort has had the highest excess mortality. Even the youngest age groups are now seeing a substantial excess, with a 9% excess in the under-50s since 2022 compared with 5% in the over-75 group.
Despite London being a younger region, the excess in London is only 3%, whereas it is higher in every more heavily vaccinated region of the UK. It should be noted that London is famously the least vaccinated region in the UK by some margin. Studies comparing regions on a larger scale show the same thing. Studies from the Netherlands, Germany and the whole world each show that the highest mortality after vaccination was seen in the most heavily vaccinated regions.
So we need to ask: what are people dying of? Since 2022, there has been an 11% excess in ischemic heart disease deaths and a 16% excess in heart failure deaths. In the meantime, cancer deaths are only 1% above expected levels, which is further evidence that this is not simply some other factor that affects deaths across the board, such as failing to account for an ageing population or a failing NHS. In fact, the excess itself has a seasonality, with a peak in the winter months. The fact that it returns to baseline levels in summer is a further indication that this is not due to some statistical error or an ageing population alone.
Dr Clare Craig from HART—the Health Advisory & Recovery Team—first highlighted a stepwise increase in cardiac arrest calls after the vaccine roll-out in May 2021. HART has repeatedly raised concerns about the increase in cardiac deaths, and it has every reason to be concerned. Four participants in the vaccine group of the Pfizer trial died from cardiac arrest compared with only one in the placebo group. Overall, there were 21 deaths in the vaccine group up to March 2021, compared with 17 in the placebo group. There are serious anomalies about the reporting of deaths in this trial, with the deaths in the vaccine group taking much longer to report than those in the placebo group. That is highly suggestive of a significant bias in what was supposed to be a blinded trial.
Toggle showing location ofColumn 564
An Israeli study clearly showed that an increase in cardiac hospital attendances among 18 to 39-year-olds correlated with vaccination, not with covid. There have now been several post-mortem studies demonstrating a causal link between vaccination and coronary artery disease leading to death up to four months after the last dose. We need to remember that the safety trial was cut short to only two months, so there is no evidence of any vaccine safety beyond that point. The decision to unblind the trials after two months and vaccinate the placebo group is nothing less than a public health scandal. Everyone involved failed in their duty to the truth, but no one cares.
The one place that can help us understand exactly what has caused this is Australia, which had almost no covid when vaccines were first introduced, making it the perfect control group. The state of South Australia had only 1,000 cases of covid across its whole population by December 2021, before omicron arrived. What was the impact of vaccination there? For 15 to 44-year-olds, there were historically 1,300 emergency cardiac presentations a month. With the vaccine roll-out to the under-50s, this rocketed to over 2,172 cases in November 2021 in this age group alone, which was 67% more than usual. Overall, 17,900 South Australians had a cardiac emergency in 2021 compared with only 13,250 in 2018, which is a 35% increase. The vaccine must clearly be the No. 1 suspect for this, and it cannot be dismissed as a coincidence. Australian mortality overall has increased from early 2021, and that increase is due to cardiac deaths.
These excess deaths are not due to an ageing population, because there are fewer deaths from the diseases of old age. These deaths are not an effect of covid, because they have happened in places that covid had not reached. They are not due to low statin prescriptions or undertreated hypertension, as Chris Whitty would suggest, because prescriptions did not change, and any effect would have taken many years and been very small. The prime suspect must be something that was introduced to the population as a whole, something novel. The prime hypothesis must be the experimental covid-19 vaccines.
The ONS published a dataset of deaths by vaccinated and unvaccinated. At first glance, it appears to show that the vaccines are safe and effective. However, there were several huge problems with how it presented that data. One was that for the first three-week period after injection, the ONS claimed that there were only a tiny number of deaths—the number the ONS would normally predict to occur in a single week. Where were the deaths from the usual causes? When that was raised, the ONS claimed that the sickest people did not get vaccinated and therefore the people who were vaccinated were self-selecting for those least likely to die. Not only was that not the case in the real world, with even hospices heavily vaccinating their residents, but the ONS’s own data show that the proportion of sickest people was equal in the vaccinated and the unvaccinated groups. That inevitably raises serious questions about the ONS’s data presentation. There were so many problems with the methodology used by the ONS that the statistics regulator agreed that the ONS data could not be used to assess vaccine efficacy or safety. That tells us something about the ONS.
Consequently, HART asked the UK Health Security Agency to provide the data it had on people who had died and therefore needed to be removed from its
Toggle showing location ofColumn 565
vaccination dataset. That request has been repeatedly refused, with excuses given including the false claim that anonymising the data would be the equivalent of creating it even though there is case law that anonymisation is not considered the creation of new data. I believe that if this data was released, it would be damning.
Some claim that so many lives have been saved by mass vaccination that any amount of harm, suffering and death caused by the vaccines is a price worth paying. They are delusional. The claim of 20 million lives saved is based on now discredited models which assume that covid waves do not peak without intervention. There have been numerous waves globally now that demonstrate that is not the case. It was also based on there having been more than half a million lives saved in the UK. That is more than the worst-case scenario predicted at the beginning of the pandemic. For the claim to have been true, the rate at which covid killed people would have had to take off dramatically at the beginning of 2021 in the absence of vaccination. That is ludicrous and it bears no relation to the truth.
In the real world, Australia, New Zealand and South Korea had a mortality rate of 400 deaths per million up to summer 2022 after they were first hit with omicron. How does that compare? With the Wuhan strain, France and Europe as a whole had a mortality rate of under 400 deaths per million up to summer 2020. Australia, New Zealand and South Korea were all heavily vaccinated before infection, so tell me: where was the benefit? The UK had just over 800 deaths per million up to summer 2020, so twice as much, but we know omicron is half as deadly as the Wuhan variant. The death rates per million are the same before and after vaccination, so where were the benefits of vaccination?
The regulators have failed in their duty to protect the public. They allowed these novel products to skip crucial safety testing by letting them be described as vaccines. They failed to insist on safety testing being done in the years since the first temporary emergency authorisation. Even now, no one can tell us how much spike protein is produced on vaccination and for how long—yet another example of where there is no data for me to share with the House.
When it comes to properly recording deaths due to vaccination, the system is broken. Not a single doctor registered a death from a rare brain clot before doctors in Scandinavia forced the issue and the Medicines and Healthcare products Regulatory Agency acknowledged the problem. Only then did these deaths start to be certified by doctors in the UK. It turns out the doctors were waiting for permission from the regulator and the regulator was waiting to be alerted by the doctors. This is a lethal circularity. Furthermore, coroners have written regulation 28 reports highlighting deaths from vaccination to prevent further deaths, yet the MHRA said in response to a freedom of information request that it had not received any of them. The systems we have in place are clearly not functioning to protect the public.
The regulators also missed the fact that in the Pfizer trial, the vaccine was made for the trial participants in a highly controlled environment, in stark contrast to the manufacturing process used for the public roll-out, which was based on a completely different technology. Just over 200 participants were given the same product
Toggle showing location ofColumn 566
that was given to the public, but not only was the data from these people never compared to those in the trial for efficacy and safety but the MHRA has admitted that it dropped the requirement to provide the data. That means that there was never a trial on the Pfizer product that was actually rolled out to the public, and that product has never been compared with the product that was actually trialled.
The vaccine mass production processes use vats of Escherichia coli and present a risk of contamination with DNA from the bacteria, as well as bacterial cell walls, which can cause dangerous reactions. This is not theoretical; this is now sound evidence that has been replicated by several labs across the world. The mRNA vaccines were contaminated by DNA, which far exceeded the usual permissible levels. Given that this DNA is enclosed in a lipid nanoparticle delivery system, it is arguable that even the permissible levels would have been far too high. These lipid nanoparticles are known to enter every organ of the body. As well as this potentially causing some of the acute adverse reactions that have been seen, there is a serious risk of this foreign bacterial DNA inserting itself into human DNA. Will anybody investigate? No, they won’t.
Sharethis specific contribution
I am grateful to the hon. Gentleman for giving way; I am conscious that time is tight. I recognise that he is making a very powerful case. Does he agree that the Government should be looking at this properly and should commission a review into the excess deaths, partly so that we can reassure our constituents that the case he is making is not in fact valid and that the vaccines are not the cause behind these excess deaths?
Sharethis specific contribution
I thank the hon. Gentleman for his support on this topic. Of course that is exactly what any responsible Government should do. I wrote to the Prime Minister on 7 August 2023 with all the evidence of this, but sadly I am still awaiting a response.
What will it take to stop these products? Their complete failure to stop infections was not enough; we all know plenty of vaccinated people who have caught and spread covid. The mutation of the virus to a weaker variant—omicron—was not enough, the increasing evidence of the serious harms to those of us who were vaccinated was not enough, and now the cardiac deaths and the deaths of young people are apparently not enough either.
It is high time that these experimental vaccines were suspended and a full investigation into the harms that they have caused was initiated. History will be a harsh judge if we do not start using evidence-based medicine. We need to return to basic science and basic ethics immediately, which means listening to all voices and investigating all concerns.
In conclusion, the experimental covid-19 vaccines are not safe and are not effective. Despite there being only limited interest in the Chamber from colleagues—I am very grateful to those who have attended—we can see from the Public Gallery that there is considerable public interest. I implore all Members of the House, those who are present and those who are not, to support calls for a three-hour debate on this important issue. Mr Deputy Speaker, this might be the first debate on excess deaths
Toggle showing location ofColumn 567
in our Parliament—indeed, it might be the first debate on excess deaths in the world—but, very sadly, I promise you it will not be the last.
2.57pm
The Parliamentary Under-Secretary of State for Health and Social Care
I congratulate the hon. Member for North West Leicestershire (Andrew Bridgen) on securing this important debate. I only have five minutes of this 30-minute debate to respond. I will try to cover all the points if I can.
Can I start by acknowledging that the hon. Member is correct that we have seen an increase in excess deaths in the last year? However, I disagree with his analysis, because the causes that he refers to simply do not bear out the statistics that we have. There has been a combination of factors contributing to the increase in excess deaths, including, in the last year, high flu prevalence, the ongoing challenges of covid-19, a strep A outbreak and conditions such as heart disease, which he touched on, diabetes and cancer. Because we had had virtually a lockdown of routine health services over a two-year period, many people are now coming forward with increased morbidity and mortality as a result.
I will start with winter flu. The number of positive tests last year peaked at 31.8%, the highest figure seen in the last six years. Interim analysis from the UKHSA indicates that the number of deaths in England associated with flu was far higher than pre-pandemic levels, so the excess deaths due to flu last winter are, sadly, part of the answer.
The hon. Member touched on the independent body, the ONS. Its figures show that the leading cause of death in England is still dementia, which accounts for about 10% of all deaths. It also looks at the cause of excess deaths. If we look at the figures as of June this year, the top three causes of excess deaths are respiratory illnesses, dementia and ischaemic heart disease, which is often caused by an increase in cholesterol, smoking or not having a blood pressure check. There are a number of reasons, and they are often chronic conditions that people have had for years, or in some cases for decades; they are not acute illnesses.
In the three minutes I have left to respond, I will touch on some of the points that the hon. Member made. First, on the importance of vaccination, it is very
Toggle showing location ofColumn 568
easy to say that there is a prevalence of high rates of covid vaccination in people who have died. That is correct: when 93.6% of the population have had at least one dose of the vaccine, there will be a high rate of vaccination in excess deaths. That is different from causality. I completely agree with the hon. Member that there is a high prevalence rate, but that is not the same as saying that vaccination is the cause of those deaths.
The Office for National Statistics has looked at this, and those who have been vaccinated have generally had a lower all-cause mortality rate than unvaccinated people since the introduction of the booster in 2021. A recent study in Singapore looked at unvaccinated patients who had recovered from covid, and showed that those patients had a 56% higher risk of cardiac complications a year later than those who were vaccinated. There is conflicting data on this issue, and I am not necessarily disagreeing with the hon. Member, but I think we need to have a robust conversation about it, not to assume that one side necessarily has all the answers.
I will touch on a couple of points that the hon. Member made about vaccine safety. The regulator has been taking account of those who report adverse events, and I encourage anyone who has had a side effect from any of the vaccines to use the yellow card system and report it to their GP. When those side effects have been reported, the MHRA has taken action. In April 2021, the MHRA reacted to rare cases of concurrent thrombosis and thrombocytopenia following the AZ vaccine, which resulted in adults under 30 not being offered that vaccine. In May 2021, that was increased to adults under 40. With regard to the mRNA vaccine specifically, following reports of a link between covid vaccines and myocarditis, the Commission on Human Medicines conducted an independent review in June 2021, which found that the incidence of that side effect was rare: between one and two cases per 100,000. When there are concerns, we absolutely must investigate them. There is no doubt about that.
We had a debate earlier this afternoon about those who have experienced rare side effects from the vaccine. We do have the vaccine damage payment scheme, which offers a payment of £120,000 if that is shown to be—
Read Next Article…
Smoking Gun Evidence That the COVID Vaccines Are Behind Skyrocketing Excess Deaths
#VaccineGenocide
Data from the popular Our World In Data showing the course of the vaccine roll-out compared to daily excess deaths, in different countries, reveals shockingly consistent, high correlations between excess deaths and vaccination rates. The data corroborates the conclusions of many doctors, pathologists, and scientists that the mRNA Covid genetic manipulators- so-called vaccines – are the direct cause of much of the extraordinary rise in deaths worldwide.
Vaccine injury and death claims at the US government’s Countermeasures Injury Compensation Program, or CICP, have skyrocketed by over 3,000% since the 2021, almost all from the COVID vaccines (NBC News station report video below.)
NBC News Atlanta: US Government Vaccine Injury Program Overwhelmed by COVID Vaccine Injury Claims
The World Health Organisation (WHO) and global data show that in 2022, about 10 million more people died around the world than would ordinarily be expected, long after COVID had subsided and most of the world had taken the “vaccines.” In the US in the later part of 2021, deaths among working -age people jumped 40%, most of it non-COVID, an astronomical number which was blacked out in the major media.
Below source: USA Today, “More young Americans are dying – and it’s not COVID. Why aren’t we searching for answers?”


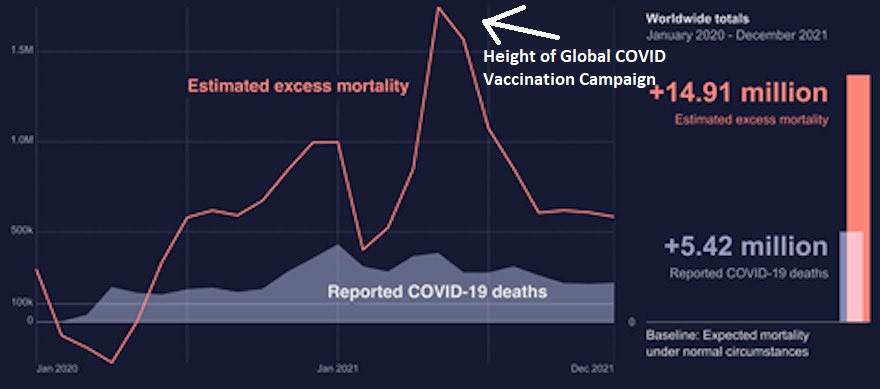
Below source: WHO.int (CLICK FOR LARGER IMAGE)
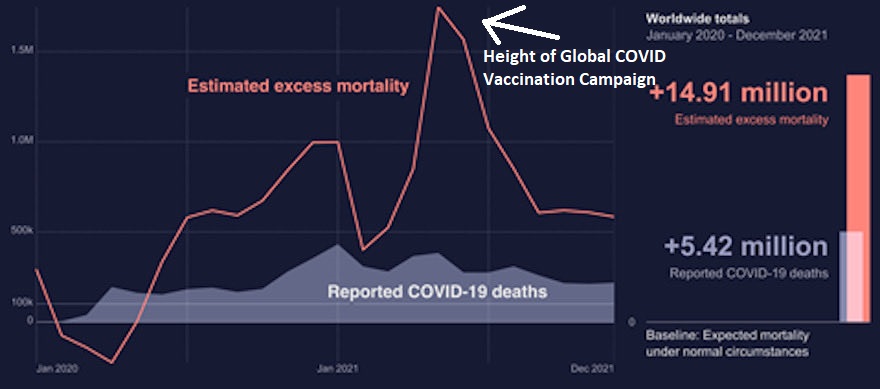
Excess mortality is the number of people who die of all causes which is over and above what would be expected, since the number remains very stable from year to year. Usually the number varies by no more than one percent from the previous year, depending on the demographic make-up of a population. Aging Baby Boomers in the US add about 40,000 to the total of about 3 million each year.
On its website, WHO deceptively tries to equate all recent excess mortality as “COVID-related,” even though these deaths include accidents, homicides, and any cause whatsoever.
About 17% more people have died globally than the historic average of about 58 million people per year, since the start of 2020, or about 34 million more people, but only 6.9 million of these deaths are from COVID.
Year Total Global All-Cause Deaths Source
2017 56.9 M
2018 57.6 M
2019 58.4 M
2020 69.9 M
2021 69.1 M
2022 69.2 M
Such an unexplained, astronomical increase all-cause deaths is getting hard to hide, as Internet searches now turns up articles such as a USA Today piece “More young Americans are dying – and it’s not COVID. Why aren’t we searching for answers?” Of the mainstream media only Dr. Drew is inviting guests, such as Columbia University Professor Spiro Pantazatos and former Blackrock fund manager Ed Dowd, who argue that the COVID vaccines are responsible. Tucker Carlson has also broken the silence.
___________________________________________________________________________
Also Read: House Bill Aims to Strip Away Pharma’s Liability Protections from Injuries and Deaths (Daily Clout)
___________________________________________________________________________
In the world of athletics, the International Olympic Committee reported that between 1966 and 2004, an average of 29 pro athletes each year died suddenly, “predominantly caused by pre-existing congenital cardiac abnormalities.” But since the COVID vaccine roll-out, nearly 1,400 pro athletes have died in 2021, 2022, and 2023 alone, as of August 2023. This is an enormous over ten-fold jump in magnitude, per year.
Long before excess all-cause deaths began to increase, many doctors and scientists, such as cardiologist Dr. Peter McCullough, were pleading to the public that the vaccines were causing the extraordinarily high number of post-vaccination deaths. Presidential candidate Robert F. Kennedy Jr.’s website Children’s Health Defense has also been asking questions in articles such as “Global Excess Mortality Rates — Where’s the Investigation?”
Below: “Dr. Peter McCullough: “Beyond Any Shadow of a Doubt,” The Vaccines Are Causing Death” (view at Rumble)
Renowned London Cardiologist Says mRNA COVID Shots Have Caused “Unprecedented Harms” And Must Be Suspended (view at Rumble)
Global data shows 27 million more global deaths from all other causes since 2020 than from COVID. At the same time, COVID deaths were so liberally counted that at times they included even people who had died of gunshot wounds. The non-COVID deaths amount to a worldwide holocaust, hiding in plain sight. By way of comparison, world military deaths for all of World War II are estimated at 21 – 25 million.
Total Global All-Cause Excess Deaths (Blue) Vs. COVID Deaths (Red,) in Millions (CLICK FOR LARGER IMAGE)

Our World in Data shows that, in country after country, increases in excess deaths from all causes corresponds closely to day-to-day and week-to-week rates of COVID vaccination. to an alarming degree. Anyone can reproduce the charts for themselves upon some mastery of the website.
Since the roll-out of the COVID vaccines, in the US over 35,000 deaths and millions of adverse events have been recorded into the CDC’s Vaccine Adverse Event Reporting System (VAERS). a 1,500% increase in yearly death reports which ordinarily average less than 200 per year for all vaccines combined since 1994.
VAERS Reported Deaths by Vaccine Type, 1988 – 2021 (CLICK FOR LARGER IMAGE)

Number of deaths reported to VAERS through 2021, number now over 35,000. Below source

Not all countries with high vaccination rates and new, extraordinarily high non-COVID, all cause death rates show the uncanny match between day-to-day vaccination rates and higher mortality, but these deaths, such as in the UK, must nevertheless be explained, rather than roundly ignored by government and media, as if by design. This is especially so since for the first time in medical history, such deaths are targeting younger, working age people.
WHO Non-COVID, All-Cause Excess Deaths and Vaccination Rate Data Corroborates Autopsies
The data showing the relationship between all-cause deaths and vaccination rates reflects the methodology of Columbia University Professor Spiro Pantazatos, who analyzed independent data sets and found that the higher the rate of vaccination, the higher the rate of excess deaths from all causes in relevant time periods.
Many forensic pathologists, such as the late Professor Dr. Arne Burkhardt, MD, have concluded from autopsies that the mRNA COVID vaccines, actually genetic manipulators, are directly responsible for many of the sudden, unexplained deaths now being acknowledged by the major media, government, and medical establishment, who are attempting to lay blame on causes such as climate change.
Top world-known cardiologists, such as London cardiologist Dr Aseem Malhotra and Dr. Peter McCullough, the latter the most scientifically published cardiologist in the world, have long warned of irreversible heart damage from the mRNA injections, and urged they be withdrawn from use. In August of 2021, a US Army Flight Surgeon Lt. Col. Dr. Theresa Long, recommended that all vaccinated pilots under her care be grounded, due to serious and well-known effects on the heart muscle which could cause heart attacks in flight. Many other doctors joined Lt. Col. Long’s 2021 lawsuit against the Biden administration for mandating the shots.
[Links to doctors’ calls for halts to mass “vaccinations,” partial list: 1, 2, 3, 4, 5. ]
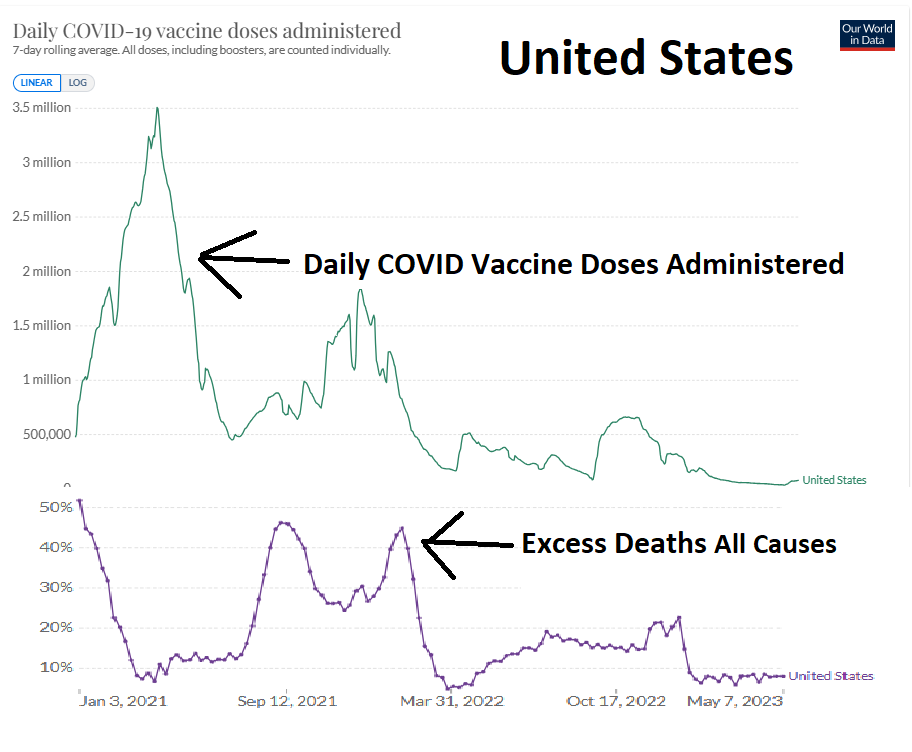
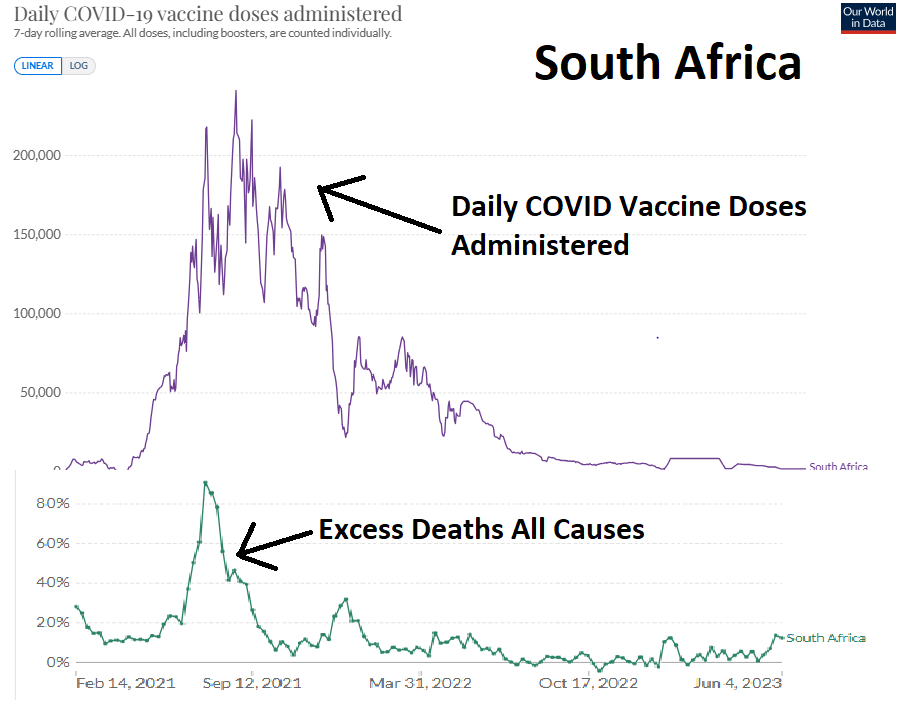
In the charts below, the data strongly indicates that as vaccinations go up, excess mortality from all causes goes up. COVID deaths have remained flat. In other words data from around the world shows that the higher the number of COVID shots given, the higher the number of people who die from non-COVID, all cause deaths.
Below: Timeline of excess deaths and COVID vaccination rates in various countries. Source of data: Our World In Data (CLICK ON IMAGE FOR LARGER IMAGE)





In the US, in the latter half of 2021, excess deaths among persons under 49 was as high as 40%, according to life insurance company data.
Short Sample COVID Vaccine Injuries, Early 2021, Over 35,000 VAERS Reports (view at Rumble)
Documented COVID Vaccine Injuries Compilation, by Henry Benedict (Rumble)
In the UK, portable refrigerated morgue units have made a comeback as hospital morgues overflow.
The major media has painstakingly hidden all of this, what would ordinarily be a story of the century. The deafening silence of the powerful is further evidence of nefarious intent.
New @WHO data on excess mortality shows that excess deaths peaked with the COVID-19 vaccine rollout. Even with billions of doses given, excess deaths do not fall back to normal levels and remain above 500k/month!@AlexBerenson @Johnincarlisle #COVID #COVID19 #coronavirus pic.twitter.com/JWqMrI3LS7
— Ben (@USMortality) August 3, 2023
The organization Mortality Watch reports that for Americans ages 0- 24, excess deaths are higher than they were at the height of COVID in 2020, by a shocking average of about 20%.
Source: Mortality Watch

Spates of articles in the major media seem designed to obscure the trend of high excess mortality following the COVID vaccination roll-out. One of the most common highlights the statistic that Red counties and states in the US have higher COVID death rates, with the inference intended that lower vaccination rates in these areas are responsible.
The articles neglect to mention that Red counties have for decades had higher death rates from all causes than Blue, mostly metropolitan areas, due to health factors such as greater obesity and smoking, and the locations of the best university teaching hospitals tending to be in the cities.
Although many peer-reviewed and non-peer reviewed studies have firmly concluded that the COVID vaccines are anything but “safe and effective” and are the direct cause of many deaths, this information is censored on the Internet and major media. Even a peer-reviewed study in a journal such as the prestigious BMJ – The British Medical Journal – which concluded that for younger people, the mRNA vaccines harmed 20x more people than they helped, is impossible to find in an Internet search for vaccine dangers, unless you already know the exact title.
Google-owned Youtube even openly declares that any information which contradicts “local health authorities or the World health Organization” is censored, no matter how distinguished the opposing source. In one instance, Youtube removed a video compilation consisting of only mainstream news reports on COVID vaccine injury. (COMPILATION HERE.)
Below: Youtube censorship notice.


The December 2022, peer-reviewed study in the BMJ, the second oldest medical science publication in the world next to The Lancet, states unequivocally that the mRNA shots (made by Pfizer and Moderna) are:
“likely to cause net expected harms to young healthy adults—for each hospitalisation averted we estimate approximately [18.5 serious adverse events]…“
In October 2022 Professor Spiro Pantazatos of Columbia University discussed, on the Dr. Drew Show, his research findings that the more COVID vaccine doses had been administered in a given region, the more adverse events were reported, making it all but certain that the vaccines were the direct cause of the adverse events. Prof. Pantazatos then estimated that by the end of 2021 actual deaths caused by the vaccines were in the hundreds of thousands.
COVID Vaccine-Injured Rally, Los Angeles, posted by on June 22, 2022 (View at Rumble)
But someone like Dr. Peter Hotez, a familiar face on TV pushing the vaccines and attacking everyone opposing them as terrorists, comes up in any search on the vaccines. It was recently revealed that Hotez had received funding from Anthony Fauci which then was shared with Chinese military scientists potentially involved in the development of COVID-19.
Worries are still strong among mRNA vaccine opponents that damage from the vaccines is only beginning to show. The average time for bringing any new drug or vaccine to general use is 10 years, and so no medium to long-term side effects are yet known. What is known is that the government, media, and medical establishment lied about everything COVID from start to finish, and so everything one may think they know about the so-called vaccines must be re-evaluated, as well as whom to believe or not believe about “misinformation.” [END ARTICLE]
Related:
House Bill Aims to Strip Away Pharma’s Liability Protections from Injuries and Deaths (Daily Clout)
Autopsies Show Direct Causal Link Between Unexpected Deaths and COVID Vaccines
Dr. John Campbell, World excess deaths, no debate
___________________________________________________________________________
COVID Vaccine Victim Information
Search Twitter by #VaccineInjuries and #VaccineGenocide
Real Not Rare Facebook page.
“Anecdotals” (documentary)
“Safe and Effective” (documentary)
World Council for Health: Covid-19 Vaccine Pharmacovigilance Report
1,000+ Peer Reviewed Articles On COVID Vaccine Injuries
Reuters: COVID Vaccine Injury Claims Skyrocket 16-Fold to 5400
Links to doctors’ calls for halts to mass “vaccinations,” partial list: 1, 2, 3, 4, 5.
___________________________________________________________________________
Science Alert: Unexpected Deaths in The US Are Rising at an Alarming Rate, June 14, 2023
Epoch Times (REPRINT): 2022 Excess Deaths All Around the World Raise an Alarm, Sept. 9, 2022
We Now Have A Clear Estimate Of The Rate Of Vaccine Injuries, by Dr. Robert Malone
It Was Cold Blooded Murder: How to Indict Bill Gates and Stop the WEF Agenda 2030

VIDEO: How COVID Vaccines Kill You, Immune Self-Attack: Pathologist Dr. Arne Burkhardt, Universities of Hamburg, Berne and Tübingen, EU Parliament 2023 (view at Rumble) (more on this…)
COVID Vaccine Victim Information
Search Twitter by #VaccineInjuries and #VaccineGenocide
Real Not Rare Facebook page.
“Anecdotals” (documentary)
“Safe and Effective” (documentary)
World Council for Health: Covid-19 Vaccine Pharmacovigilance Report
1,000+ Peer Reviewed Articles On COVID Vaccine Injuries
Reuters: COVID Vaccine Injury Claims Skyrocket 16-Fold to 5400
Links to doctors’ calls for halts to mass “vaccinations,” partial list: 1, 2, 3, 4, 5.
Brave Denver Police Officer Crippled by Mandated Vax, Breaks Down on TV ‘Can’t Carry My Kids to Bed’
Related posts:
Views: 0
 Posted in
Posted in  Tags:
Tags: 

















{kind=link}
{kind=link}
{kind=link}